TL;DR
- Most longevity programs can show biomarker movement, but not definitive proof of better long-term clinical outcomes.
- Aging clocks, NAD⁺ therapies, plasma-based interventions, and regenerative treatments remain scientifically interesting but incompletely validated for broad longevity claims.
- The strongest path forward is structured interpretation, clinician-in-the-loop governance, and longitudinal outcome tracking tied to meaningful clinical endpoints.
What Are Longevity Clinics Actually Measuring?
Most longevity clinics measure some combination of epigenetic clocks, metabolic markers, inflammatory markers, hormone panels, wearable data, and subjective wellness outcomes. These tools can support risk stratification and program monitoring, but they do not by themselves prove that a protocol improves healthspan.
That distinction defines the current evidence gap. A clinic can show that a lab value changed, a score improved, or a biological age estimate declined, but that is not the same as proving fewer cardiovascular events, less frailty, or longer healthy life.
Why Are Biomarkers Not Enough to Prove Efficacy?
Aging is multi-system, gradual, and difficult to measure through a single endpoint. That is why researchers often rely on surrogate biomarkers to estimate whether an intervention is moving in the right direction before harder outcomes such as disability, multimorbidity, or mortality can be observed.
The problem is that most aging biomarkers are not yet validated surrogate endpoints in the regulatory sense. A marker may correlate with risk and still fail to show that changing the marker causes a meaningful clinical benefit.
Are Aging Clocks Valid Surrogate Endpoints?
Not yet. Some aging clocks predict mortality and morbidity better than chronological age, and newer phenotypic tools can outperform traditional risk models in observational datasets. But that does not mean lowering a clock score through a clinic program has been proven to reduce disease burden or extend healthspan.
This is where the literature diverges. Some researchers see clocks as promising future trial tools, while others argue their practical value over established clinical risk scores remains uncertain.
Why Is Long-Term Clinical Evidence So Hard to Generate?
The trial design challenge is substantial. To prove that a longevity intervention works, a study must run long enough, include enough participants, and use endpoints that matter clinically rather than relying only on biomarker movement.
Commercial clinics rarely operate in that format. Many deliver multi-domain programs that combine nutrition, exercise, supplements, pharmacology, infusions, and regenerative procedures at the same time, which makes attribution difficult. If outcomes improve, it can be hard to isolate which component produced the effect.
There is also a structural incentive problem. Many interventions can already be offered in cash-pay settings before definitive outcome evidence exists, which weakens the commercial pressure to run large, expensive, long-duration trials.
Which Longevity Interventions Have the Strongest Evidence?
The evidence base is uneven. Interventions tied to established disease indications tend to have stronger human outcome data, while broad anti-aging claims usually rest on biomarkers, mechanistic reasoning, or small studies.
What Do NAD⁺ Therapies Actually Prove?
Human studies on NAD⁺ precursors such as NR and NMN show target engagement and generally acceptable short-term safety, but outcome effects are mixed, modest, or null depending on the endpoint.
That creates a clear gap between program design and clinical evidence. NAD⁺ IVs are widely offered, but they are not supported by trials showing reduced morbidity, improved function at scale, or longer healthspan.
What Do Plasma Exchange Studies Show?
Plasma-based interventions are among the most discussed areas in longevity medicine because the underlying biology is compelling. One recent trial reported reductions in multi-omics biological age and improvements in selected functional measures with therapeutic plasma exchange plus IVIG.
But the broader picture is mixed. Other studies have failed to show sustained reversal of epigenetic age, and some findings suggest protocol details matter substantially. At this stage, plasma exchange should be viewed as promising but unresolved rather than established.
Where Do Stem Cell Therapies Have Real Evidence?
The clearest human evidence for mesenchymal stromal or stem cell therapies is in indication-specific use cases such as knee osteoarthritis. Meta-analyses of randomized trials support improvements in pain and function in those settings, though long-term structural benefit remains less certain.
That is very different from proving generalized anti-aging effects. Clinics may reasonably discuss regenerative evidence in orthopedic contexts, but broad longevity claims are not supported by equivalent outcome data.
Why Do Repurposed Drugs Have a Stronger Evidence Base?
Repurposed drugs such as metformin, SGLT2 inhibitors, and GLP-1 receptor agonists are supported by large disease-specific evidence bases, especially in cardiometabolic care. That makes them more credible than interventions marketed primarily through mechanism or biomarker change alone.
Even so, an important distinction remains. These drugs may improve pathways relevant to aging, but that is not the same as proving they slow aging itself in otherwise healthy adults.
Why Are Regulators Cautious About Longevity Claims?
Regulators do not currently recognize aging as a stand-alone therapeutic indication. That means interventions must usually be developed around specific diseases, syndromes, or clinically accepted functional endpoints.
FDA- and EMA-aligned frameworks also set a high bar for biomarker qualification. A surrogate endpoint must be convincingly linked to real clinical benefit in the intended setting, and most aging biomarkers do not yet meet that threshold.
This is why many longevity claims remain commercially visible but medically unvalidated. Clinics may be able to show signal, but not yet the level of proof required for regulatory-grade efficacy claims.
Where Is the Evidence Strongest Today?
The most credible evidence in longevity medicine is not concentrated in the most novel interventions. It is strongest in evidence-backed prevention, cardiometabolic risk reduction, structured lifestyle programs, and therapies already proven in defined clinical indications.
That does not make newer interventions irrelevant. It does mean that the closer an offering is to established preventive medicine or indication-specific evidence, the stronger its current clinical footing tends to be.
What Should Longevity Clinics Look For?
Clinics should distinguish carefully between promising biomarkers and proven outcomes. Biomarker-guided programs can be useful, but outcome claims should remain conservative unless they are supported by validated endpoints and transparent longitudinal data.
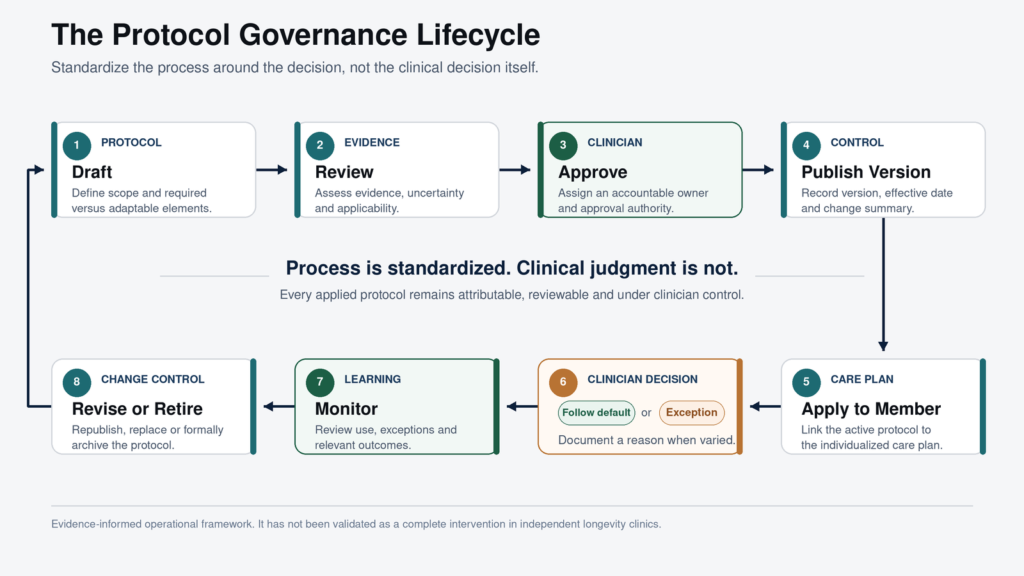
The strongest operating models will standardize protocols, track members over time, and publish outcomes in ways that can be independently assessed. In a market crowded with claims, governance, standardization, and evidentiary discipline are becoming strategic differentiators.
What Should Investors Look For?
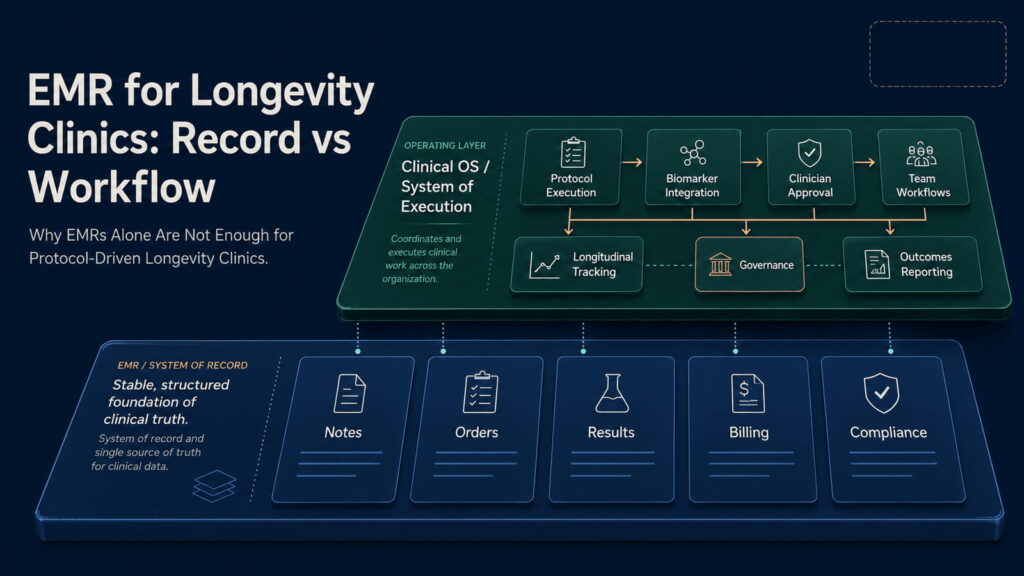
Investors should evaluate longevity clinics as evidence-generating systems rather than premium wellness brands. The core questions are whether the clinic can standardize care, collect longitudinal data, and build a credible path from biomarker tracking to measurable outcomes.
The biggest risk is mistaking surrogate movement for durable clinical value. The strongest opportunities are likely to sit with operators and operating infrastructure that can turn fragmented longevity programs into governed, measurable, outcome-oriented systems.
What Will Define the Next Phase of Longevity Clinics?
The next phase of the market will likely be defined by better biomarker validation, better trial design, and better clinical governance. Hybrid endpoints that combine biomarkers, function, and disease outcomes may help make studies more practical without abandoning clinical relevance.
Clinics that already operate with standardized workflows, transparent oversight, and longitudinal reporting will be better positioned as that evidence base matures. Until then, the core challenge remains unchanged: most longevity clinics can measure change, but very few can yet prove definitive clinical outcomes.
HolistiCare provides clinical decision-support infrastructure; it is not a licensed medical provider or electronic health record. All diagnostics, care protocols, and clinical decisions remain exclusively the responsibility of qualified healthcare professionals. Insights generated by HolistiCare’s AI engine are for clinical and informational use only and do not constitute medical advice, diagnosis, or treatment.
References
- A Framework for an Effective Healthy Longevity Clinic
- Validation of biomarkers of aging
- Endpoints for geroscience clinical trials: health outcomes, clinical endpoints, and biomarkers
- Information on FDA review of geroscience-related IND applications
- Table of Surrogate Endpoints That Were the Basis of Drug Approval or Licensure
- Surrogate Endpoint Resources for Drug and Biologic Development
- Biomarkers and Surrogate Endpoints in Drug Development
- Opinions and letters of support on the qualification of novel methodologies
- NAD⁺ supplementation for anti-aging and wellness
- Clinical Evidence for Targeting NAD Therapeutically
- Clinical trial and multi-omics analysis demonstrating therapeutic plasma exchange effects
- Human plasmapheresis and epigenetic age findings
- Young donor plasma transfusion and age-related outcomes
- Clinical efficacy and safety of stem cell therapy for knee osteoarthritis
- Stromal cell-based injection therapies for knee osteoarthritis
- Geroscience-guided repurposing of FDA-approved drugs to target aging
- Clinical Trials Targeting Aging
- Pharmacological interventions in human aging