Clinical note: This article is an editorial on clinical operations and architecture for longevity practices. HolistiCare.io is a clinical decision-support platform; it does not diagnose or treat patients. Clinical implementation of any workflow should be performed by licensed clinicians in accordance with applicable laws and professional standards.
In the high-stakes world of longevity medicine, data is not merely a record of what happened; it is the roadmap for future care. Yet, in 2026, the vast majority of functional medicine and longevity clinics are operating on Electronic Health Records (EHRs) designed for a different era and a different purpose. This article analyzes the architectural limitations of popular “Practice Management” platforms when applied to precision medicine and outlines the necessity of a “Clinical Intelligence” layer to achieve true scalability and proactive capability.
The “Digital Filing Cabinet” Paradox
As we move through 2026, the longevity sector has matured from a niche bio-hacking community into a standardized medical discipline. However, the operational backbone of most clinics has not kept pace.
I frequently consult with Medical Directors who are frustrated. They have invested heavily in platforms widely recognized in the functional space—systems that are excellent at scheduling, billing, and basic charting. Yet, when these Directors attempt to perform population health analysis or track longitudinal biomarker trends across a patient panel, they hit a wall.
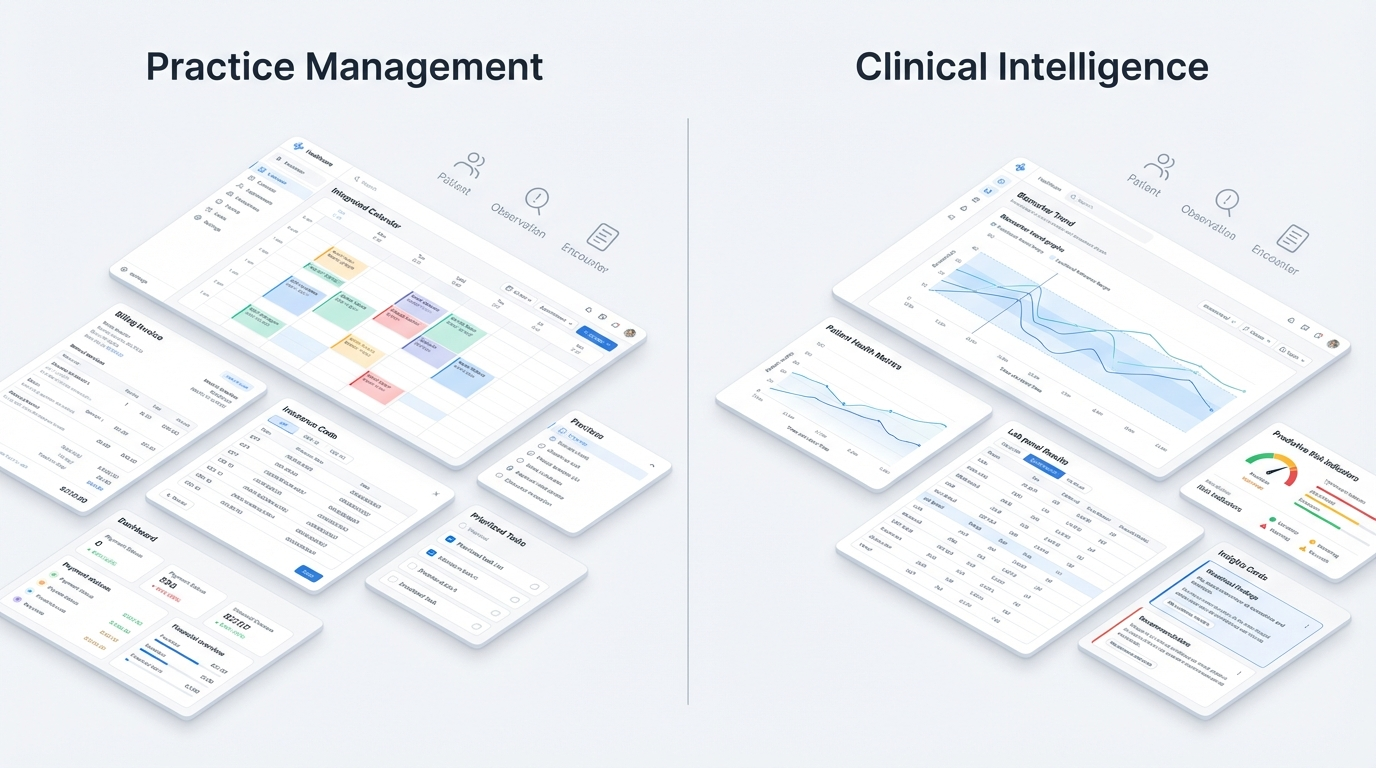
They are discovering the fundamental difference between Practice Management (PM) and Clinical Intelligence (CI).
The dominant legacy players in our space (often referred to in comparative conversations involving platforms like Cerbo or Practice Better) were architected primarily to solve administrative friction. They excel at ensuring the intake form is sent, the calendar is synced, and the credit card is charged. These are vital functions. However, strictly speaking, they function as “Digital Filing Cabinets.” They digitize paper processes but often retain the limitations of paper: data is static, siloed, and retrospective.
For a General Practitioner treating acute illness, this is sufficient. For a Longevity Physician managing the rate of biological aging, it is an operational ceiling.
The Architectural Divergence: “Blobs” vs. Structured Data
To understand why a generic EHR fails a longevity clinic, we must look at the database level.
1. The Unstructured “Blob” Problem
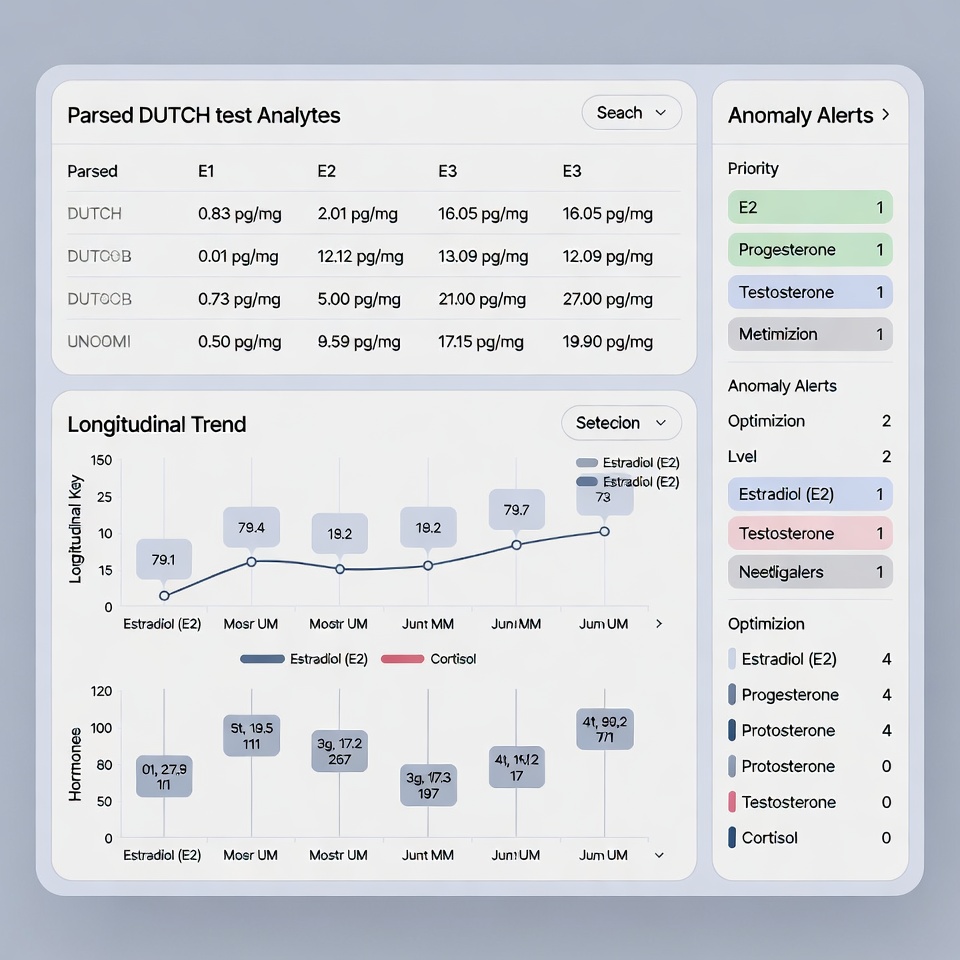
In many legacy systems, when a specialty lab report (e.g., a DUTCH test or a GI-MAP) arrives, it is ingested as a PDF attachment. To the software, this file is an “unstructured blob” (Binary Large Object). The system knows that a document exists, and it knows who it belongs to, but it does not know what is inside the document.
The data points—Estradiol, Cortisol metabolites, Pyroglutamate—are trapped inside the image. They cannot be graphed, they cannot be queried, and they cannot trigger automated alerts.
2. The Structured JSON Standard
HolistiCare.io operates on a fundamentally different schema. We utilize Structured Data ingestion. When a lab result arrives, it is parsed into individual data fields (JSON objects).
- Legacy System View:
Patient_File_Jan_2026.pdf(File Size: 2MB) - HolistiCare View:
{"Biomarker": "HbA1c", "Value": 5.2, "Unit": "%", "Date": "2026-02-02", "Delta_vs_Baseline": -0.1}(synthetic example for illustrative purposes)
This distinction is the difference between having a library of books you can only look at, versus having a search engine that can index every word on every page.
The Clinical Consequences of “Flat” Data
When data is unstructured, the burden of intelligence shifts entirely to the physician’s cognitive load. This creates three critical risks for the scaling clinic:
Risk A: The Longitudinal Blindspot
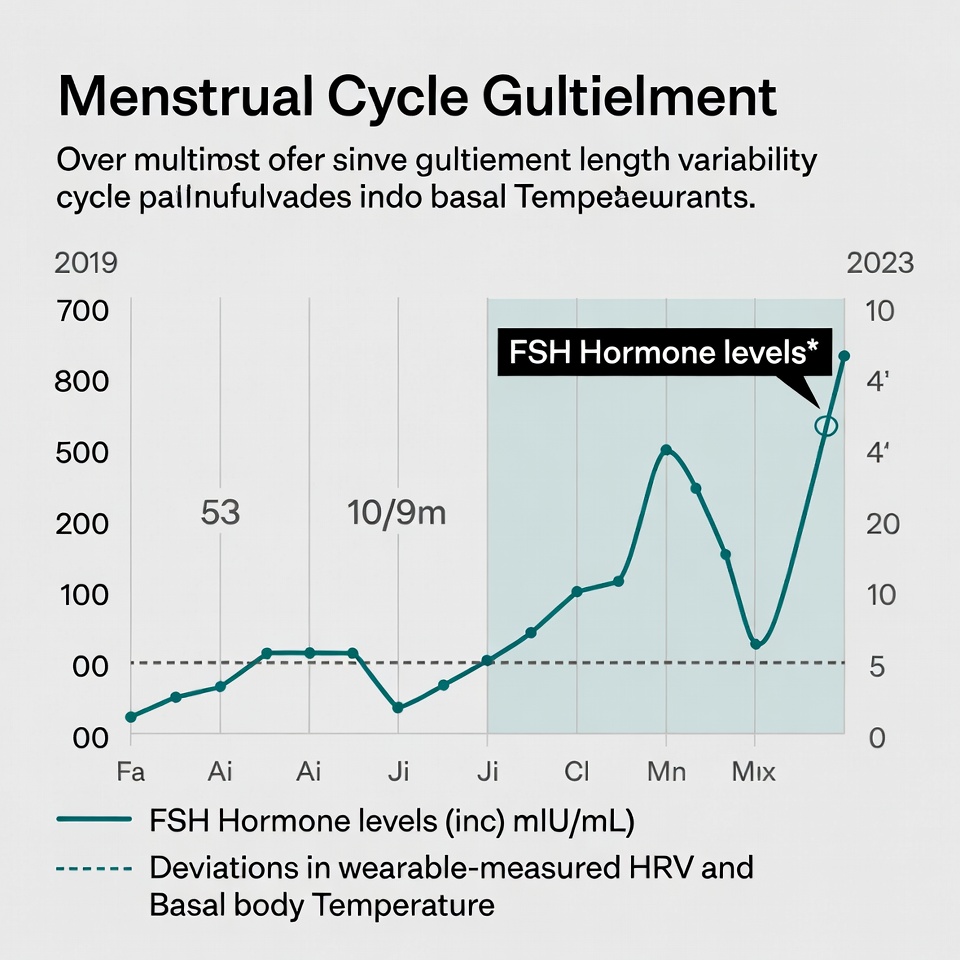
Longevity medicine is the study of “Delta” (change over time). A single fasting insulin reading of 5.0 uIU/mL is good. But if the patient was at 2.5 uIU/mL six months ago, that is a 100% increase—a red flag indicating metabolic dysfunction.
In a legacy PM system, spotting this trend requires the physician to open two separate PDF files and mentally compare the numbers. Across a panel of 200 patients, this manual comparison is impossible to sustain. HolistiCare’s Clinical Intelligence visualizes trends, computes Delta values, and surfaces alerts when trajectories exceed clinician-defined thresholds or protocol rules.
Risk B: The “Sub-Clinical” Drift
Standard EHRs rely on reference ranges provided by the lab (e.g., Labcorp or Quest). These ranges are statistical averages of the population—a population that, statistically, is metabolically unhealthy.
A longevity clinic does not aim for “Normal”; it aims for “Optimal.”
- Lab Range for TSH: 0.45 – 4.50 uIU/mL
- Functional/Longevity Target: 1.0 – 2.0 uIU/mL
Legacy systems trigger an alert (Red Flag) only when the patient crosses the pathological threshold (4.50). HolistiCare supports custom “Optimal Ranges” and will surface clinician-configured alerts when values deviate from defined targets, enabling earlier clinical review and potential preventive strategies.
Risk C: The Interoperability Silo
Many clinics utilize a “Frankenstein Stack”: one app for scheduling, one for nutrition tracking (like Cronometer), one for wearables (Oura/Whoop), and one for labs.
Without a central Clinical Intelligence layer to ingest and normalize these streams via API (Application Programming Interface), the data never meets. You cannot see how a patient’s Deep Sleep (from Oura) correlates with their Cortisol (from the DUTCH test) because those data points live in different universes.
The Solution: The “Hybrid” Stack Strategy
We are not necessarily advocating for a “Rip and Replace” strategy. Migration is painful. Instead, we advocate for a Layered Architecture.
In this model, your legacy system (Cerbo, Practice Better, etc.) remains the engine for Practice Management. HolistiCare.io is deployed as the Clinical Intelligence Layer that sits on top.
How it works technically:
- Bi-Directional Sync: We utilize HL7 FHIR (Fast Healthcare Interoperability Resources) standards to pull patient demographics and appointment types from your PM system.
- Clinical Workflows: The physician and medical staff operate primarily inside HolistiCare during the consult, utilizing the advanced visualization and AI-assisted charting tools.
- Data Write-Back: Encounter notes and finalized care plans are pushed back into the PM system for billing compliance and record retention.
ROI: The Metric of “Time-to-Insight”
The ultimate ROI of this transition is Time-to-Insight.
Example Time-to-Insight (Illustrative):
- Manual Workflow: ~30 minutes to review 3 PDFs, draft a note, and explain trends to the patient.
- HolistiCare Workflow: ~8 minutes to review pre-populated dashboard, analyze AI-assisted insights, and discuss with patient.
Note: Actual results vary by clinic volume and workflow configuration.
By efficiently managing consult time, a clinic can either see more patients or, more likely in the longevity model, dedicate that time to higher-value relationship building and strategy.
Conclusion: Future-Proofing the Clinic
Clinics that treat data as a strategic asset are better positioned for the 2026–2030 cycle. While administrative tools are necessary for keeping the lights on, Clinical Intelligence tools are necessary for supporting patient health—and retention.
References & Citations
- Centers for Medicare & Medicaid Services (CMS). “Interoperability and Patient Access Final Rule.” Federal Register, 2020.
- Mandl, K. D., & Kohane, I. S. (2016). “Time for a Patient-Driven Health Information Economy?” New England Journal of Medicine, 374(2), 105-106.
- Topol, E. J. (2019). Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again. Basic Books.
- HIMSS (Healthcare Information and Management Systems Society). “The Definition of Interoperability.” HIMSS Dictionary of Health Information Technology Terms, 2024 Edition.
- Office of the National Coordinator for Health Information Technology (ONC). “Cures Act Final Rule: Information Blocking.” HealthIT.gov, 2025 update.
Disclaimer: The information in this article is for educational and informational purposes only and does not constitute medical, legal, or financial advice. References to products, vendors, or clinical strategies are for comparative purposes and do not imply endorsement. HolistiCare.io is a B2B clinical decision-support platform and does not independently diagnose, prescribe, or treat medical conditions. Clinicians are responsible for all clinical decisions and for ensuring compliance with federal, state, and local regulations. Results discussed are illustrative; actual outcomes vary.



What do you think?
[…] data to prospective clinical data. This is where the value of a system like HolistiCare’s Clinical Intelligence Layer becomes structurally apparent — because this layer requires the ability to aggregate, interpret, […]