How to Automate Lab Report Analysis in Clinics
Executive Summary: In clinical practice, manual lab report analysis remains a significant bottleneck, consuming valuable clinician time and introducing variability in interpretation. This inefficiency delays patient care and limits scalability in functional medicine and longevity-focused clinics. Automation offers a pragmatic solution by streamlining data processing, standardizing interpretation, and integrating actionable insights into clinical workflows. Leveraging automation reduces human error, improves turnaround times, and frees clinicians to focus on patient-centered decision-making rather than data entry and manual review. Successful automation requires thoughtful implementation that respects clinical nuance and maintains flexibility for individualized care. This includes selecting appropriate software tools, integrating with existing electronic health records, and designing workflows that enhance rather than disrupt clinical operations. Ultimately, automating lab report analysis augments clinical judgment with reliable, consistent data handling. For clinic owners aiming to optimize efficiency and patient outcomes, adopting automation is a strategic imperative aligned with the evolving demands of functional medicine and longevity care.
intro
Current lab practices
Most clinics rely on a hybrid of manual chart review, PDF copying, and human interpretation. Physicians or nurses pull up lab PDFs, transcribe values into templates or clinical notes, and annotate clinically relevant abnormalities. Some practices use spreadsheets or basic middleware to aggregate values, but interpretation and prioritization remain clinician tasks. This model works at very small scale but becomes a throughput problem as patient volume, panel complexity, and test variety increase.
Time constraints
Time is the scarcest resource. Reviewing panels—metabolic, micronutrient, hormonal, specialty tests—takes minutes per report when thorough. Multiply that by hundreds of patients and you have substantial uncompensated labor. Clinics either accept slower turnaround, frustrating patients and delaying treatment, or triage superficially and risk missing subtleties. Administrative staff can extract values, but clinical interpretation requires clinician oversight, creating a bottleneck.
Workflow impact
The manual model fragments workflow: labs arrive asynchronously, staff flag results, clinicians chase context, and decisions are deferred. This fragmentation increases cognitive load, creates chart backlog, and forces rushed telephonic or asynchronous follow-up. It also drives burnout—time spent parsing numbers is time not spent on patient counseling, complex decision-making, or practice development.
problem
Manual inefficiency
Manual extraction and transcription are error-prone and slow. Copy-paste errors, misplaced decimal points, and misread units are common. Clerical work consumes clinical time better spent on differential diagnosis and treatment planning. In episodic billing models, time spent on data wrangling is uncompensated overhead.
Interpretation variability
Interpretation depends on clinician experience, specialty bias, and local practice habits. Two clinicians can read the same ferritin, TSH, or cortisol result and reach different conclusions about significance or next steps. Lack of consistent interpretive rules leads to variable patient advice, inconsistent follow-up ordering, and difficulty standardizing care pathways.
Delayed feedback
When labs pile up, communication slows. Delayed messaging erodes patient trust and decreases adherence. Patients expect prompt, clear next steps; when timelines stretch, engagement drops. For time-sensitive issues—abnormal electrolytes, severe anemia, or infection—delay is clinically unsafe.
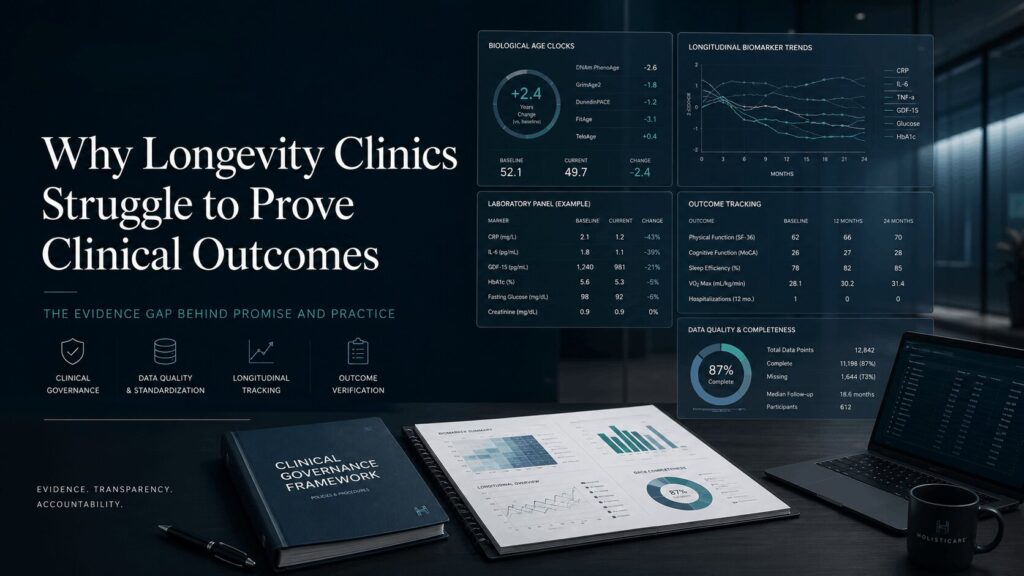
Data overload
Modern panels produce more numbers than a clinician can mentally synthesize in every encounter. Longitudinal trends, ratio calculations, and cross-panel correlations are easy to miss. Without automated summarization, actionable patterns—progressive iron decline, subtle thyroid drift, or metabolic shifts—can be buried in noise.
automation
Standardized extraction
Automation starts with reliable data capture: structured extraction from lab interfaces (HL7, API) or robust OCR parsing of PDFs when interfaces are absent. Standardizing units, normal ranges, and result metadata at ingestion prevents downstream confusion. Consistent extraction enables downstream algorithms and dashboards to operate on normalized fields rather than ad-hoc text.
Algorithmic interpretation
Rule-based logic and transparent algorithms codify common interpretive patterns: flagging critical thresholds, calculating ratios (eGFR trends, LDL/HDL), and generating prioritized problem lists. Algorithms should be simple, auditable, and configurable—clinicians must adjust thresholds and override suggestions. Avoid black-box scoring for safety-critical decisions; use algorithmic outputs as structured suggestions, not mandates.
EHR integration
Automation must fit into the EHR or clinical platform to avoid parallel systems. Ideally, extracted data and interpretive summaries flow into the chart as discrete data elements, not images or attachments. Integration reduces duplicate data entry, enables clinical decision support at point of care, and preserves audit trails. Where direct integration isn’t possible, middleware can push structured notes and discrete lab values upstream.
Error reduction
Properly implemented automation reduces transcription errors, enforces unit consistency, and provides prompt critical-value alerts. It frees humans to audit exceptions rather than perform rote extraction, reducing both silent errors (missed trends) and loud errors (mis-keyed values), improving reliability of follow-up recommendations.
implementation
Software selection
Choose tools prioritizing clinical transparency, interoperability, and configurability. Required features include HL7/FHIR or dependable API connectivity, robust parsing for non-standard labs, configurable rule engines, audit logs, and clinician-friendly reporting. Avoid flashy AI claims without clear explainability and validation. Confirm vendor support for mapping local reference ranges and customizing clinical rules.
Workflow redesign
Automation shifts work; it does not eliminate it. Redefine roles so clinicians review algorithmic summaries and handle exceptions, while staff triage routine follow-ups. Map the workflow end-to-end: lab receipt → automated extraction → algorithmic summary → clinician review queue → patient communication. Limit dual documentation by ensuring summaries write back to the EHR as discrete data.
Staff training
Train clinicians and staff on what automation does and does not do. Emphasize interpreting algorithmic flags, overriding recommendations, and correcting mis-parsed values. Provide quick reference guides and hands-on sessions; expect a learning curve and plan for temporary increased review time while confidence builds.
Data security
Labs and patient results are protected health information. Ensure encryption in transit and at rest, role-based access controls, and business associate agreements with vendors. Audit trails and traceability of every parsed value back to source files are essential for compliance and clinical safety.
Quality monitoring
Implement routine audits: random chart checks, discrepancy tracking between original lab documents and parsed values, and monitoring clinician overrides. Use audits to refine parsing rules and interpretive thresholds. Establish KPIs (parsing accuracy, time-to-notification, clinician override rate) and review regularly.
CTA
Assess workflows
Conduct a rapid process audit: measure average time per report, transcription error incidence, and backlog size. Identify manual steps adding no clinical value and suitable for automation. Baseline metrics are necessary to evaluate impact post-deployment.
Explore tools
Compile a shortlist of vendors meeting interoperability and transparency criteria. Run a technical proof-of-concept including your common lab formats. Prioritize tools allowing clinician control over interpretive rules rather than closed AI models.
Pilot projects
Start small: pilot a single high-volume panel (e.g., metabolic, thyroid, vitamin D) to reveal integration and workflow issues with limited risk. Use pilot to tune rules and staff roles before broader rollout.
Measure gains
Track time saved per report, backlog reduction, time-to-notification changes, and clinician satisfaction. Monitor patient outcomes indirectly—did faster interpretation affect follow-up or treatment? Use metrics to justify scale-up.
Automation should augment, not replace, clinician judgment. HolistiCare.io combines clinical experience with configurable automation components so clinics can standardize repetitive tasks while preserving individualized care plans. For a practical starting point rather than vaporware, consider a short pilot targeting a single panel and measuring key metrics.
Automate now to enhance your clinic’s efficiency and patient care quality.