Abstract
The wellness industry generated $5.6 trillion in global revenue in 2022. It is also, by any objective clinical measure, one of the most ethically compromised commercial landscapes in modern healthcare. Supplement stacks with fabricated efficacy claims. Detox protocols with no mechanistic basis. Influencer-physicians performing clinical authority on platforms optimized for emotional engagement rather than evidentiary rigor.
This brief makes a contrarian argument: the dysfunction of the wellness market is not a threat to the serious clinician. It is a structural opportunity. In a market saturated with noise, credibility is the scarcest commodity. This is a systematic framework for building, protecting, and deploying Ethical Authority as the primary competitive instrument in the functional medicine and longevity space — and for doing so without compromising clinical standards, manufacturing consent through social media performance, or mistaking reach for trust.
Authority cannot be purchased. It can only be built — methodically, publicly, and on an evidentiary foundation that withstands professional scrutiny.
I. The Diagnosis: What Is Actually Wrong With the Wellness Industry
Before we can build an alternative, we must be precise about what we are building against. Vague critique of ‘the wellness industry’ is itself a form of intellectual laziness. Let us be specific.
1.1 The Three Structural Pathologies
The wellness market suffers from three distinct, overlapping pathologies. Each one is commercially self-reinforcing, which is precisely why it persists.
Pathology One: The Unfalsifiability Loop
The most commercially durable wellness claims are constructed to be unfalsifiable. ‘Support your gut health.’ ‘Optimize your cellular energy.’ ‘Balance your hormones.’ These are not clinical hypotheses. They are semantic constructions that sound clinical but specify no measurable endpoint, no mechanism, and no testable prediction.
This is not accidental. Unfalsifiable claims cannot be disproven, which makes them legally safer and commercially more durable than specific, evidence-based assertions. The practitioner who claims a supplement ‘supports metabolic function’ is legally and clinically insulated from accountability in a way that the practitioner who claims it ‘reduces fasting glucose by 12% in insulin-resistant adults’ is not.
The clinical operator who wants to compete ethically in this space faces a structural disadvantage: honest specificity is more vulnerable than vague implication. The corrective, as we will argue, is to convert that vulnerability into a trust signal.
Pathology Two: The Authority-Performance Confusion
Social media algorithms do not reward expertise. They reward emotional engagement — specifically, the emotions of aspiration, fear, and belonging. The clinician who posts a video expressing genuine clinical nuance will be systematically outperformed by the clinician who posts a confident, oversimplified claim delivered with conviction.
This creates what we term the Authority-Performance Confusion: the conflation of social visibility with clinical credibility. A physician with 800,000 followers on a short-form video platform is not, by that metric alone, authoritative. They are merely visible. Authority is earned through a different mechanism entirely.
A physician with 800,000 followers is not authoritative. They are merely visible. Authority is earned through a different mechanism entirely — one that social media algorithms actively penalize.
Pathology Three: The Supplement-Industrial Complex
The functional medicine space has developed a commercially problematic dependency on supplement revenue. When a clinician’s income is structurally tied to the sale of proprietary supplement protocols, a conflict of interest exists that the patient is rarely informed of and that the clinician frequently fails to consciously acknowledge.
A 2022 analysis in JAMA Internal Medicine found that nearly 40% of supplements marketed with claims of clinical benefit contained ingredients not supported by peer-reviewed evidence [1]. The clinician who recommends these products — even in good faith — is participating in an integrity deficit that, when eventually exposed, will contaminate the credibility of every practitioner in the category.
These three pathologies create, for the serious clinician, a remarkable opportunity. The floor of credibility in this market is catastrophically low. The marginal return on genuine ethical authority is therefore exceptionally high.
II. What Ethical Authority Actually Is (And Is Not)
The term ‘authority’ is used loosely in marketing discourse to mean anything from social proof to celebrity endorsement. We use it in its original, more precise sense: the legitimate right to be believed on the basis of demonstrable competence and verifiable integrity.
Ethical Authority, as we define it at HolistiCare, is the compound effect of three independently verifiable attributes:
What Ethical Authority is not:
- It is not humility theater. Performing modesty on social media — ‘I’m just asking questions’ — while selling a $300/month supplement protocol is a manipulation, not a virtue.
- It is not credential inflation. Listing every certification, fellowship, and board membership in a bio is a signal of insecurity, not authority. Authority does not require a long list of abbreviations.
- It is not consensus deference. Authority does not mean agreeing with every institutional guideline. It means having a defensible, evidence-grounded position — and being willing to articulate why you diverge from consensus when you do.
- It is not platform absence. We are not arguing that clinicians should avoid digital presence. We are arguing that the architecture of that presence should be calibrated to build trust, not to maximize engagement.
III. The Architecture of Ethical Authority: Five Structural Pillars
Ethical Authority is not a disposition. It is a designed system. It must be constructed, maintained, and protected with the same intentionality that one applies to clinical protocol design. What follows is the five-pillar architecture we have developed at HolistiCare.
Pillar One: The Evidentiary Foundation
The first pillar is the most fundamental and the most frequently neglected: your clinical positions must be grounded in a documented, updatable evidence base that you can produce on demand.
This means more than generally being familiar with the literature. It means:
- Maintaining a living evidence library. For every clinical claim your practice makes — every biomarker interpretation, every therapeutic recommendation, every mechanism assertion — there should be a corresponding body of evidence you can cite. Not anecdote. Not clinical impression. Peer-reviewed literature, ideally from Tier 1 journals with independent replication.
- Acknowledging the limits of the evidence. The most counterintuitive move in this market is to publicly acknowledge where the evidence is weak, contested, or absent. This is not a commercial liability — it is the highest-yield trust signal available to a clinician. The practitioner who says ‘the data on this intervention is preliminary, here is what we know and here is what we don’t know’ is categorically more credible than the one who presents every recommendation with equivalent confidence.
- Updating your positions when evidence evolves. The clinician who publicly revises a recommendation in response to new data is demonstrating exactly the epistemic behavior that distinguishes science from dogma. Document it. Explain it. This is a content asset, not a liability.
The practitioner who publicly says 'the evidence on this is preliminary' is not losing a sale. They are building the trust that makes every future recommendation 10 times more persuasive.
Pillar Two: Protocol Systematization
The second pillar connects directly to HolistiCare’s core architectural thesis: ethical authority requires that your clinical decision-making be systematized, documented, and reproducible — not dependent on the real-time cognitive performance of an individual clinician.
There are two reasons this is an authority issue, not merely an operations issue.
First: a practice whose clinical outcomes depend on the personal genius of its founder cannot be audited, improved, or scaled. A practice whose clinical outcomes are produced by a documented protocol can be measured, validated, and refined. Only the latter can claim, with any intellectual integrity, that it is evidence-based.
Second: when a patient harm occurs — and in any sufficiently active clinical practice, adverse events will occur — the existence of a documented protocol is both a legal protection and an ethical one. It demonstrates that clinical judgment was not arbitrary. It provides an auditable record of the reasoning process. The Hero Doctor who operates from intuition and experience has no such defense.
The Hero Trap in Ethical Terms
The Hero Doctor model is not merely a business risk — it is an ethical one. When a practice's clinical quality is inseparable from the personal attention of its founder, the practice is making an implicit promise to every patient that it cannot reliably fulfill. What happens to the patient scheduled with the associate physician, the covering provider, the telehealth extension? If the protocol lives only in the founder's head, the quality differential is real, invisible, and unaddressed.
Protocol systematization is not a compromise of care quality. It is the precondition for delivering consistent care quality at any scale beyond a solo practitioner's personal panel.
Pillar Three: Radical Transparency in Commercial Relationships
The third pillar addresses the conflict-of-interest problem directly. The wellness industry’s credibility problem is substantially a disclosure problem. Practitioners sell supplements they profit from, recommend tests from labs in which they have financial relationships, and present commercially motivated recommendations as pure clinical judgment.
The ethical authority play is simple and strategically powerful: disclose everything, and structure your commercial relationships to survive disclosure.
This means several concrete things:
- Make your conflict disclosures visible, not buried. If you have a dispensary relationship with a supplement company, say so on your website, in your intake materials, and before you make the recommendation. The practitioner who proactively discloses is not vulnerable to the accusation of concealment.
- Design your protocol to be conflict-neutral. Wherever possible, structure your clinical recommendations around interventions that do not generate secondary revenue for your practice. When a commercially beneficial recommendation also happens to be the correct clinical recommendation, document the evidence basis explicitly so that the recommendation’s integrity is visible.
- Separate your supplement revenue from your clinical authority. If you offer a dispensary, treat it as a convenience function — not a clinical revenue center. The moment your supplement sales become a meaningful percentage of practice revenue, your clinical judgment is structurally compromised regardless of your intentions.
Pillar Four: The Asymmetric Content Strategy
We do not advocate for social media abstinence. We advocate for a fundamentally different architecture of digital presence — one optimized for trust accumulation rather than engagement metrics.
The conventional social media strategy for wellness practitioners is built on volume, emotional resonance, and the parasocial relationship. Post daily. Share your journey. Be relatable. Build a community. This strategy can generate significant following and meaningful revenue, but it has a structural ceiling: it scales reach without scaling authority. At some threshold of audience size and content frequency, the practitioner inevitably compromises clinical rigor to maintain engagement. The algorithm demands it.
We call our alternative the Asymmetric Content Strategy, because it inverts the conventional optimization target:
The clinical audience that can actually pay for high-value services — corporate health programs, executive longevity protocols, physician-referred complex patients — does not discover their providers on short-form video. They discover them through professional networks, institutional reputation, referral relationships, and long-form content that demonstrates clinical depth.
A single well-researched 3,000-word clinical brief — such as this one — will generate more qualified inbound interest over 18 months than 200 social media posts will generate in the same period. The economics of asymmetric content compound over time in a way that engagement-driven content does not.
Pillar Five: Institutional Signal Amplification
The fifth pillar is the mechanism by which individual clinical authority is amplified into institutional authority — the transition from ‘I trust this doctor’ to ‘I trust this clinic’s system.’
Institutional signal amplification operates through a specific set of mechanisms:
- Peer publication and citation. Even a single published case series, outcomes report, or methodology paper in a peer-reviewed journal — regardless of impact factor — represents an institutional signal of a fundamentally different category than any social media presence. It signals that your methodology has survived external peer review. For many sophisticated patient populations, this is decisive.
- Professional organization engagement. Speaking at conferences, serving on committees, and contributing to specialty organization publications does not generate consumer reach. It generates professional credibility — the trust of referring physicians, insurance panels, and corporate HR departments. These are the institutional gatekeepers to high-value patient populations.
- Outcome data publication. The most powerful institutional signal available to a functional medicine practice is published outcome data from its own patient population. This requires that outcomes be systematically measured — which returns us to Pillar Two. You cannot publish what you have not measured. You cannot measure what you have not systematized. The pillars are interdependent.
- Strategic media placement. A single well-placed quote in a credible trade publication — NEJM, Health Affairs, Medical Economics — carries more institutional authority than a year of social media output. The practitioner who understands how to position for earned media in professional publications is operating in a different market than the practitioner optimizing for consumer social metrics.
IV. The Commercial Architecture of Ethical Authority
We have described what Ethical Authority is and how to build it. Now we address the question that sophisticated clinicians will correctly raise: does it actually generate revenue? Is this a framework for building a commercially viable practice, or a framework for building a professionally respected but financially marginal one?
The answer is unequivocal. Ethical Authority, properly deployed, is the highest-yield commercial strategy available in the functional medicine and longevity space. The mechanism is not complicated.
4.1 The Trust Premium
In markets characterized by information asymmetry — where the buyer cannot easily evaluate the quality of what they are purchasing before committing — trust functions as the primary determinant of price tolerance. Healthcare is the archetypal information-asymmetric market.
A patient who trusts their clinician — not because of marketing, but because of demonstrable competence, transparent disclosure, and consistent intellectual integrity — is significantly more price-insensitive than the average consumer. They are also significantly less price-sensitive to competitive alternatives. The cost of switching away from a trusted clinician is perceived as higher than the cost of switching away from a merely competent one.
The Trust Premium is not a marginal pricing advantage. Research on high-trust professional service relationships consistently demonstrates that trusted advisors command 25-40% higher fees than comparable competitors without established trust relationships — and retain clients at significantly higher rates [2].
4.2 The Referral Compounding Effect
The most durable revenue architecture in professional services is the referral network, and referral networks are built on trust, not reach. The wellness influencer with 500,000 followers generates revenue through volume — a low-priced product or program sold to a large, diffuse audience. The trusted clinician with an Ethical Authority positioning generates revenue through depth — high-value services sold to a smaller, highly qualified patient population that refers aggressively to peers of equivalent socioeconomic and health sophistication.
The math is instructive. Consider two practitioners:
The influencer model is not non-viable. It is simply not the architecture of a sustainable, high-margin clinical enterprise. It is a media business wearing a clinical costume.
4.3 The Regulatory Moat
The wellness market is under increasing regulatory scrutiny. The FTC has significantly expanded enforcement against unsubstantiated health claims in the past five years, and state medical board action against physicians making unsupported claims in commercial contexts is increasing [3]. The FDA has indicated expanded oversight of functional and health-forward food product claims.
The practitioner who has built Ethical Authority — whose claims are documented, whose evidence base is citable, whose commercial relationships are disclosed — is structurally insulated from this regulatory risk. They are operating in compliance with standards that the broader market has not yet adopted. When regulatory enforcement increases, as it predictably will, the practitioner with Ethical Authority positioning does not face an adaptation cost. Their competitors do.
This is the Regulatory Moat: competitive protection that accumulates passively as ethical practice creates documented compliance while market-wide enforcement pressure eventually raises the floor to where you already are.
V. The HolistiCare Infrastructure Layer: Systematizing Authority
The five pillars described above are architectural principles. Their implementation requires infrastructure. A clinician who intends to build Ethical Authority through systematized, outcome-measured, transparently documented clinical practice cannot do so using documentation-first EHR infrastructure designed for billing compliance and chart notes.
This is not a peripheral observation. It is structurally central. Consider what Ethical Authority requires at an operational level:
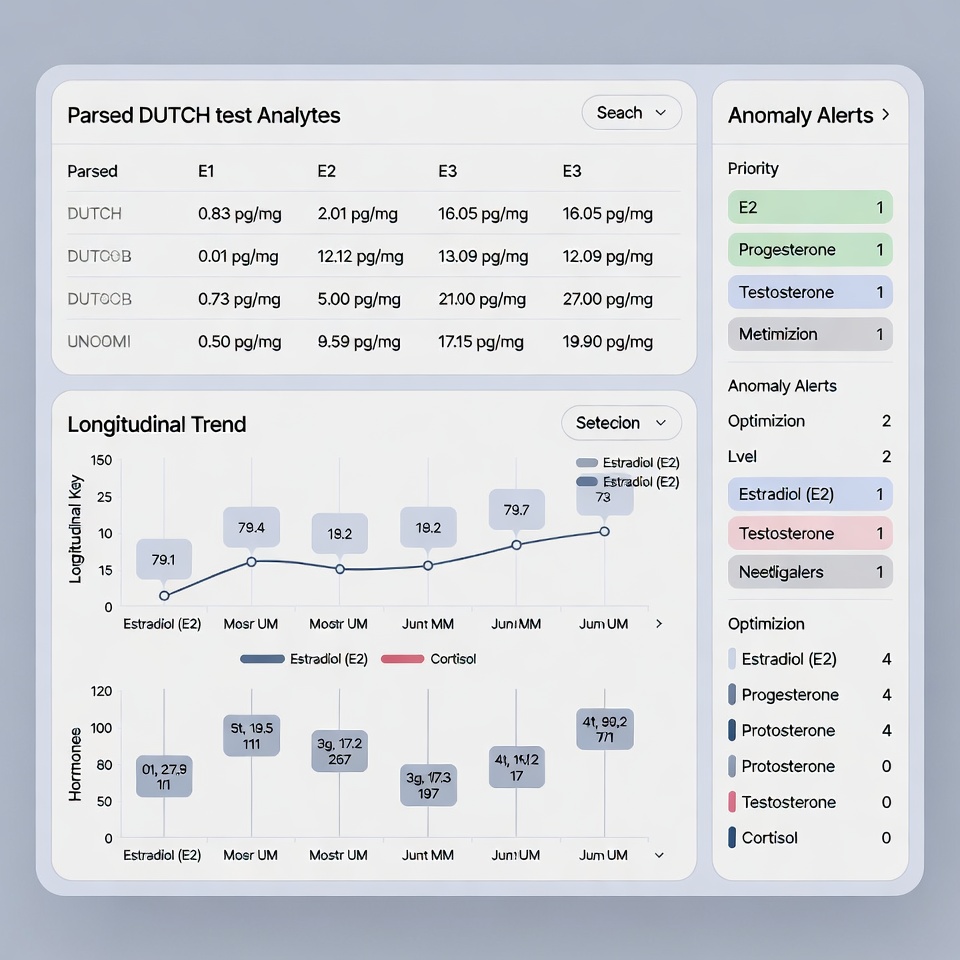
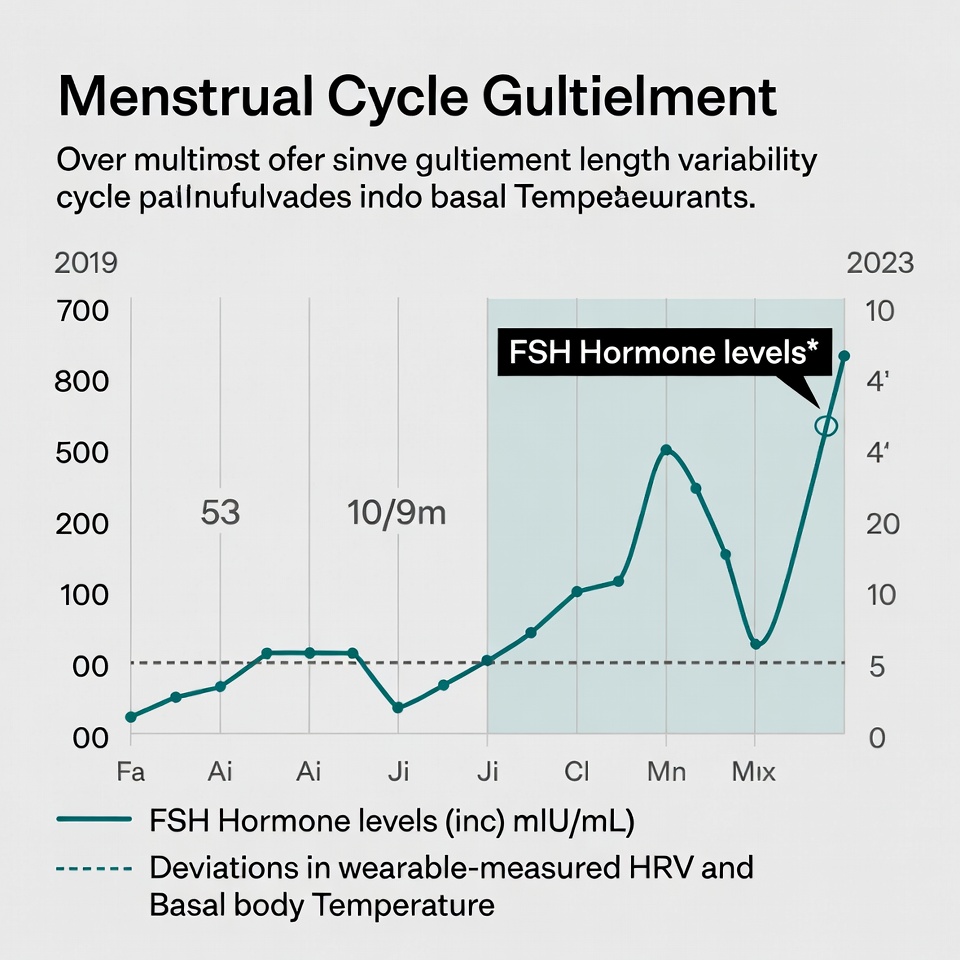
- Biomarker trending and longitudinal correlation. The clinician who claims to practice evidence-based functional medicine must be able to demonstrate — to patients, peers, and regulators — that their recommendations are correlated with measurable biomarker outcomes. This requires a clinical intelligence layer that ingests, normalizes, and trends lab data over time. Legacy EHR systems document lab results. They do not correlate them.
- Protocol standardization and version control. A systematized practice requires that clinical protocols are documented, version-controlled, and consistently applied. When a protocol is updated in response to new evidence, the update must be traceable. This is not a documentation function — it is a decision-support function. HolistiCare’s Clinical Intelligence Layer maintains protocol integrity across a multi-provider practice without requiring individual practitioners to carry the protocol in their heads.
- Outcome data aggregation for publication readiness. Publishing practice-level outcome data requires that data be structured, de-identified, and analyzable. The practice that wants to publish its results cannot do so if its data lives in unstructured chart notes in a documentation-first EHR. It requires a clinical data infrastructure designed around measurable endpoints.
- Patient-facing transparency dashboards. One of the highest-yield implementations of Ethical Authority is giving patients direct, interpretable visibility into their own biomarker trends, protocol adherence, and outcome trajectory. This is not merely a patient satisfaction tool — it is a trust architecture. The patient who can see their own data trending in response to their protocol is not vulnerable to competitive offers from wellness influencers promising faster results. They have evidence of their own progress.
The practice that cannot show a patient their own biomarker trend over 18 months is asking for trust without offering evidence. That is not Ethical Authority. That is a faith-based clinical relationship — and it is exactly what we are arguing against.
The intersection of Ethical Authority and Clinical Intelligence infrastructure is not coincidental. They are, in the final analysis, the same thing expressed differently: the commitment to letting evidence, not performance, be the mechanism of trust.
VI. The Practical Roadmap: Building Ethical Authority in 18 Months
The following is a sequenced implementation roadmap for the clinician who wants to transition from conventional wellness positioning to Ethical Authority positioning. It is designed to be executed without abandoning existing revenue streams, compromising patient relationships, or requiring a social media presence rebuild.
Phase 1: Foundation (Months 1-3)
The first phase is internal. Nothing is published. Nothing is marketed. The objective is to build the evidentiary and operational infrastructure on which authority will rest.
- Audit your current clinical claims. For every claim your practice makes — in marketing materials, patient communications, protocol documentation — apply the following test: Can I cite a peer-reviewed source for this? If not, revise or remove it. This is a discomfort exercise. Do it anyway.
- Document your protocols. If your clinical approach cannot be written down in sufficient detail that a competent colleague could deliver consistent care from it, you do not have a system — you have a practice that depends on you. This is a protocol development exercise, not a bureaucratic one.
- Audit your commercial relationships. List every supplement company, lab, referral partner, and ancillary service provider from which your practice derives revenue. For each one, answer: Is this disclosed to patients? Is this disclosed in my marketing? Is the clinical recommendation independent of the revenue relationship? Restructure what fails this audit.
- Implement a clinical data infrastructure. If your current EHR cannot produce longitudinal biomarker trend data, aggregate outcome metrics, or structured protocol documentation, you are operating a documentation system, not a clinical intelligence system. Evaluate solutions accordingly.
Phase 2: Publication and Positioning (Months 4-9)
The second phase begins building visible authority signals. The emphasis is on depth, not volume.
- Publish one foundational long-form piece per month. This is not a blog post. It is a clinical brief: 2,000-3,500 words, with citations, structured argument, and a clearly defensible position. Distribute it through professional networks, not consumer social media. Submit for republication in specialty organization publications.
- Identify two professional conference presentations. Even a local or regional functional medicine conference provides an institutional signal of a different category than any social media output. Submit an abstract. Speak on a specific clinical topic with documented outcome data. The credibility accrual begins with the acceptance.
- Initiate a structured outcome measurement program. Select three to five clinical endpoints across your most common patient presentations. Build a measurement protocol. Begin collecting data with patient consent. This is the foundation of the outcome publication you will produce in Phase 3.
- Formalize your disclosure infrastructure. Add conflict-of-interest disclosure to your website, intake documentation, and patient communications. This feels uncomfortable. It is, in fact, the highest-trust move available.
Phase 3: Authority Compounding (Months 10-18)
The third phase is where Ethical Authority begins to generate measurable commercial returns. Referral quality improves. Fee tolerance increases. Regulatory risk diminishes.
- Submit your first outcome paper. Even a small patient cohort — 30 to 50 patients — tracked over 12 months with structured endpoints is publishable in a clinical specialty journal. The submission itself is a signal. The acceptance is a market position.
- Build your referral architecture. Identify 20 to 30 high-quality referring physicians — primary care physicians, cardiologists, endocrinologists — who serve patient populations aligned with your clinical focus. The content you published in Phase 2 is your calling card. The outcome data you have collected is your clinical proposition.
- Revise your pricing structure. If you have executed Phases 1 and 2 with rigor, your practice’s trust profile has materially improved. Reprice accordingly. The Trust Premium is real and it is now earned. Retaining your previous pricing is a commercial misalignment.
- Evaluate your social media presence with new criteria. For each platform where you have a presence, ask: Is this generating referrals from qualified sources? Is this building professional credibility? Is this consistent with the evidentiary standards I have established in other channels? If the answer is no, reallocate that time to content that answers yes.
VII. A Direct Address to the Counterargument
We anticipate a specific objection from clinicians who have built meaningful practices on conventional wellness positioning: ‘This approach is slower, harder, and less visible than what I am currently doing. Why would I change a model that works?’
The honest answer has three parts.
First: the model is working until it isn’t. Wellness market dynamics are shifting. Consumer sophistication about supplement efficacy claims is increasing. Regulatory enforcement is expanding. Platform algorithms are unstable. The practice built on influencer reach is more fragile than it appears when engagement metrics are high.
Second: the revenue ceiling of the influencer model is lower than it appears. A practice that generates $500,000 per year selling high-volume, low-margin wellness products is generating five times the administrative burden, ten times the customer service overhead, and a fraction of the margin of a practice generating the same revenue through a smaller panel of high-trust, high-value clinical relationships. The economics of depth are superior to the economics of reach at the level of practice profitability.
The practice that generates $500K per year through 4,000 supplement subscribers and the practice that generates $500K through 80 high-trust clinical relationships are not the same business. One is a media company. The other is a medical practice. They should not be confused.
Third: there is a professional integrity argument that has nothing to do with commercial optimization. We are physicians. We were trained in a tradition that places evidence and patient welfare above commercial interest. The wellness market has created enormous pressure to compromise this tradition incrementally — one unfalsifiable claim, one undisclosed supplement relationship, one emotionally resonant oversimplification at a time. Ethical Authority is not merely a market strategy. It is a professional identity choice.
The market will eventually price integrity correctly. Those who built it systematically, before the market required it, will have the position that others will spend years attempting to replicate.
VIII. Conclusion: The Authority Compound
The wellness market will not self-correct. The incentive structures that produce unfalsifiable claims, undisclosed conflicts, and performance-driven authority are too commercially powerful to dissolve without external pressure. That pressure is coming — from regulators, from consumer sophistication, and from the inevitable credibility collapse of practitioners whose authority rests on engagement metrics rather than evidence.
What we have described in this brief is not a defensive posture against that collapse. It is an offensive one. The clinician who builds Ethical Authority now is not merely protecting themselves from future market correction. They are accumulating a structural advantage that compounds over time: more qualified patients, better referral relationships, higher fee tolerance, lower regulatory exposure, and a professional reputation that survives the market cycles that erode celebrity-driven positioning.
The five pillars — Evidentiary Foundation, Protocol Systematization, Radical Transparency, Asymmetric Content Strategy, and Institutional Signal Amplification — are not aspirational principles. They are operational specifications. They require work. They require infrastructure. They require the discipline to optimize for trust over visibility when the two are in conflict.
They also require the intellectual honesty to acknowledge that the ‘Art of Medicine’ — the romanticized notion that clinical quality is an ineffable personal gift that resists systematization — is, in many of its common deployments, a rationalization for the avoidance of accountability. The clinician who says ‘my practice is too nuanced to be systematized’ is often saying ‘I prefer not to be measured.’
We prefer to be measured. We believe that every serious clinician, given the choice, shares that preference. HolistiCare exists to provide the infrastructure that makes measurement possible and authority therefore earnable.
Build it correctly. Build it patiently. The compounding will take care of the rest.
References
[1] Cohen, P. A., Avula, B., Wang, Y. H., et al. (2022). Quantity of New Dietary Supplements on the US Market and FDA Adverse Event Reports. JAMA Network Open, 5(5), e2215430.
[2] Maister, D. H., Green, C. H., & Galford, R. M. (2021). The Trusted Advisor. Simon & Schuster. (Updated 20th Anniversary Edition.)
[3] Federal Trade Commission. (2023). FTC Health Claims Report: Enforcement Actions Against Unsubstantiated Wellness and Supplement Claims, 2018-2023. FTC Bureau of Consumer Protection.
[4] Global Wellness Institute. (2023). Global Wellness Economy Monitor. GWI Research Publications.
[5] Ornish, D., Blackburn, E. H., et al. (2013). Increased telomerase activity and comprehensive lifestyle changes: a pilot study. The Lancet Oncology, 9(11), 1048-1057.
[6] Ioannidis, J. P. A. (2016). Why Most Clinical Research Is Not Useful. PLOS Medicine, 13(6), e1002049.
[7] Sackett, D. L., Rosenberg, W. M., Gray, J. A., et al. (1996). Evidence based medicine: what it is and what it isn’t. BMJ, 312(7023), 71-72.
[8] Topol, E. J. (2019). High-performance medicine: the convergence of human and artificial intelligence. Nature Medicine, 25(1), 44-56.
[9] Institute of Medicine. (2001). Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press.
[10] Brownstein, J., & Abrams, D. (2022). Integrative Medicine and the Commercialization of Wellness: Ethical Frameworks for Clinical Practice. Journal of Alternative and Complementary Medicine, 28(4), 287-295.
Legal & Medical Disclaimer:
This document is produced for educational and informational purposes by HolistiCare.io and does not constitute medical advice, clinical guidance, legal counsel, or financial consulting. The market analyses, revenue projections, and commercial frameworks presented herein are illustrative models intended for educational discussion among healthcare professionals. Individual practice outcomes will vary based on clinical context, market conditions, regulatory environment, and practitioner competence. HolistiCare.io does not guarantee specific clinical, regulatory, or commercial outcomes from implementing any strategy described in this brief. All clinical practices should be implemented under the supervision of licensed healthcare professionals in compliance with applicable state and federal regulations. Clinicians are advised to consult qualified legal, compliance, and financial professionals before making material changes to their commercial or clinical infrastructure. HolistiCare.io is a clinical intelligence software company and does not provide direct clinical services.