Personalized longevity care becomes operationally unscalable when personalization depends on manual clinician labor — undocumented judgment, ad hoc data review, fragmented follow-up, and inconsistent protocol execution — rather than on governed, repeatable operating workflows. The scalable alternative is not less personalization. It is structured process that preserves clinical judgment while standardizing everything around it.
Key findings:
- Personalization itself is not the constraint on clinic growth; how it is executed operationally is.
- Longer consultations, advanced diagnostics, and high-touch follow-up create a structural mismatch between clinical workload and available time as member volume grows.
- Biomarker panels, genomics, wearables, and lifestyle data increase clinician interpretive workload faster than most clinics’ systems can support.
- Founder-led clinical methodology is typically tacit and undocumented, making it difficult to reproduce consistently across a growing care team.
- Follow-up, adherence tracking, and retesting are frequently the hidden operational bottleneck, not the initial consultation.
- Governed standardization (structured process) and commoditized standardization (removed clinical judgment) are not the same thing — confusing them is what stalls scalable personalization.
The Operational Paradox of Personalized Longevity Care
Personalization is not the constraint on growth in longevity, concierge, and functional medicine. The constraint is how personalization gets executed.
In founder-led clinics, personalization typically runs through one person’s judgment. The founder reviews the panel, interprets the pattern, designs the protocol, and remembers to follow up. This works because the founder holds the entire clinical model in their head. It does not require documentation, because there is nothing to hand off.
That model breaks the moment a clinic adds a second practitioner, a third location, or a member cohort large enough that no single clinician can personally track every case. At that point, the absence of a governed operating workflow for longevity clinics stops being a personal habit and starts being an operational liability — and it is this gap, more than any deficiency in concierge medicine operations themselves, that defines the scale ceiling.
The evidence base on this is not specific to longevity medicine — it is specific to time-intensive, judgment-heavy clinical work in general. A BMJ Open analysis of consultation-task time found that delivering the tasks recommended in standard “10-minute consultation” guidance actually requires a median of 15.7 to 28.4 minutes, against a backdrop of 17 recommended tasks per visit. Longevity and concierge visits, which layer multi-domain biomarker review, lifestyle counseling, and protocol explanation onto a single encounter, are structurally more demanding than the conventional visits this research describes. The mismatch between clinical workload and available time is not new — it is older and better documented in adjacent care settings than in longevity medicine specifically, and it compounds when personalization runs on memory rather than process.
This is the operational paradox: the clinics best positioned to attract premium members with high expectations for continuity, clarity, and measurable progress are often the ones least equipped, structurally, to serve a growing number of them without diluting the care that earned that reputation.
How the Longevity Clinic Workflow Breaks Down as Volume Grows
A typical personalized care journey moves through seven stages. Each one has a distinct failure mode that emerges specifically at scale — not at the level of a handful of members, but once volume, team size, or program count increases.
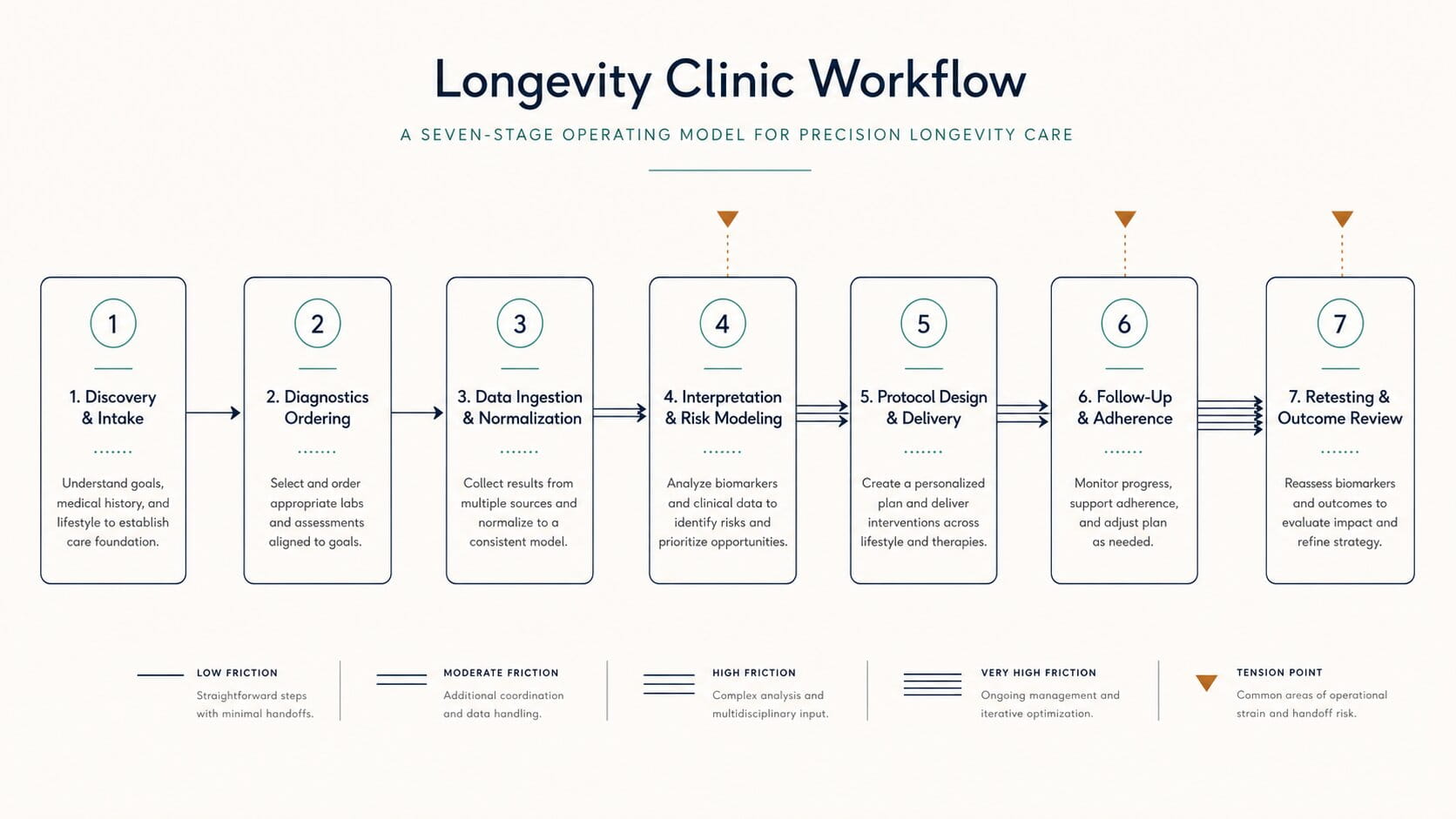
Discovery and intake
Intake in longevity and functional medicine is rarely a simple form. It requires synthesizing medical history, functional symptoms, lifestyle context, and prior diagnostics into an initial clinical picture. When this synthesis depends on a senior clinician’s personal triage — done from memory, with informal heuristics about who needs urgent attention — it does not scale. New staff have no consistent reference for how triage decisions were historically made, so they either escalate everything or miss what the founder would have flagged immediately.
Diagnostics ordering
Ordering advanced panels — metabolic, hormonal, inflammatory markers, genomics, microbiome, imaging — frequently involves coordinating across multiple labs with no shared ordering system. Research on biomarker testing integration in oncology found that the absence of EHR-integrated ordering and results workflows leads to manual handling, delays, and data-entry errors even in well-resourced clinical settings. In a smaller clinic without that infrastructure, test selection often varies by clinician — some over-order to avoid missing findings, others under-order to control member cost — and that inconsistency becomes difficult to manage once more than one practitioner is ordering panels.
Data ingestion and normalization
Lab results, genomic reports, wearable data, and lifestyle inputs arrive through different portals, formats, and cadences. Precision medicine interoperability research shows that even within hospital systems, biomarker and genomic data are inconsistently captured and frequently fail to transfer cleanly into downstream records. For more on how this plays out specifically in longevity clinic data environments, see why longevity clinic data stays fragmented. Without normalized data capture, every new data source — a new wearable, a new lab partner — adds another manual reconciliation step that consumes clinician or staff time before any clinical interpretation can begin.
Interpretation and risk modeling
This is where clinical judgment is most legitimately exercised — and where workload is most likely to overwhelm a growing team. Genomic and clinical decision-support literature notes that the routine accumulation of large data volumes in clinical records can overwhelm clinicians without yielding proportional clinical benefit, particularly absent dedicated interpretive tooling. This is the core mechanism behind what is often called biomarker interpretation overload. Founder clinicians often develop interpretive heuristics over years — pattern recognition across panels that is never written down. When a second or third clinician interprets the same data differently, the clinic has no internal reference point for which approach reflects its actual clinical standard.
Protocol design and delivery
Building a multi-domain care plan — medication optimization, supplementation, nutrition, sleep, stress, exercise — and communicating it clearly takes real time. Evidence on consultation-task time requirements already shows that delivering structured recommendations exceeds standard visit lengths in conventional primary care. Longevity protocols, which are more multidimensional, are unlikely to fit more comfortably. Without a consistent plan format, clinicians also produce protocols of varying detail and structure, which complicates handoff to coaching or care-team staff responsible for supporting delivery — undermining clinical protocol standardization before a program even reaches its first follow-up.
Follow-up and adherence
This stage generates the largest volume of unscheduled, asynchronous work — messages, check-ins, plan adjustments — and it is the stage most likely to be under-resourced because it does not appear as a discrete line item on a calendar. Research on time pressure in clinical visits found that constrained consultation time is associated with increased follow-up appointments and messaging volume, as unresolved issues spill into subsequent interactions. Reviews of wearables in clinical care similarly note that without clear workflows for translating continuous data into action, longitudinal monitoring produces high data volume with limited clinical signal — a pattern often described as data accumulating faster than clinicians can act on it.
Retesting and outcome review
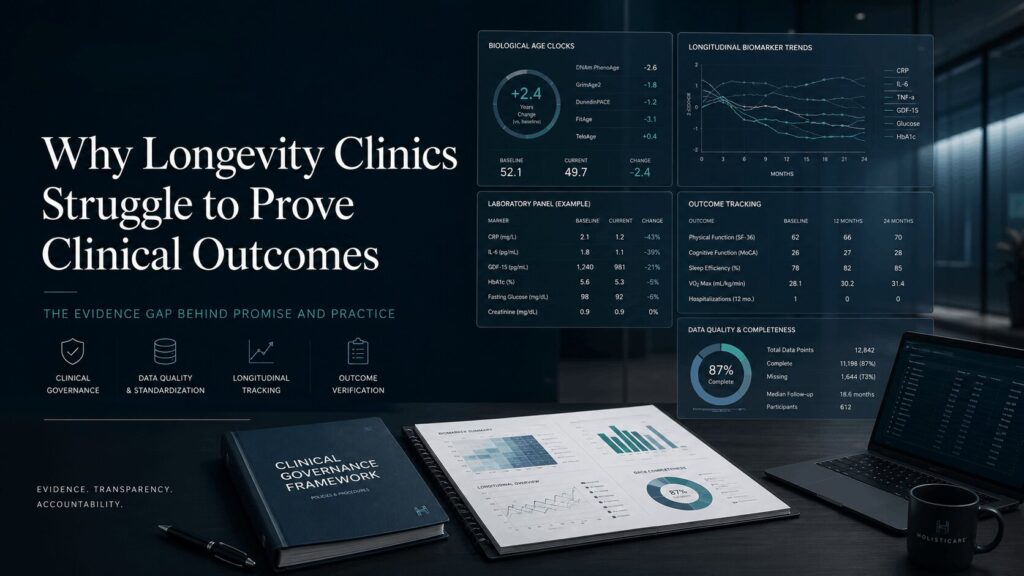
Without a defined retesting cadence, the timing and scope of follow-up panels vary by clinician preference, making capacity planning unpredictable and longitudinal comparison difficult. This is also where outcome tracking tends to break down — a clinic may be improving member biomarkers consistently, but without structured longitudinal tracking, it cannot easily demonstrate that. This issue is explored further in why longevity clinics struggle to prove clinical outcomes.
The Root Causes Behind the Scale Ceiling
The breakdowns above trace back to six distinct categories of complexity. Treating them as one undifferentiated problem — “personalization is hard” — makes the actual constraint harder to diagnose, and obscures whether a clinic’s scalability problem is clinical, operational, or both.
Clinical complexity. Longevity members frequently present with multimorbidity and multi-domain risk profiles that require integrated assessment across systems, not single-issue diagnosis. This is inherently more cognitively demanding per encounter than visit-based, single-complaint care.
Data complexity. Biomarker panels, genomics, microbiome results, continuous monitoring data, and self-reported lifestyle inputs create a multi-layered data environment. Interoperability research consistently finds that integrating these data types reliably into a shared clinical record remains technically unresolved, even in well-funded healthcare systems.
Operational complexity. Documentation and administrative burden are well-documented contributors to reduced clinical capacity. Research on EHR-related burnout shows that documentation and clerical tasks are among the strongest contributors to time pressure and reduced satisfaction among clinicians.
Staffing complexity. Personalized, biomarker-led care depends on clinicians with specialized interpretive expertise. Training pathways for this kind of judgment are rarely standardized, even within a single practice, which makes recruiting and onboarding slower than in protocol-driven care models — and makes care team coordination harder as headcount grows.
Technology complexity. Clinicians report persistent usability and interoperability shortcomings in EHR systems that disrupt rather than support complex workflows. In longevity clinics, this is compounded by the use of multiple disconnected platforms — EHR, lab portals, wearable dashboards, member apps — for what should be a single member journey.
Member adherence complexity. Longitudinal digital health research shows that adherence to self-monitoring and lifestyle interventions tends to decline over time, even among motivated participants. Sustaining engagement requires active staff attention, which adds to — rather than reduces — the operational load of follow-up.
Personalization as Clinical Judgment vs. Personalization as Manual Labor
This distinction is the conceptual center of the problem, and most clinics have not made it explicitly.
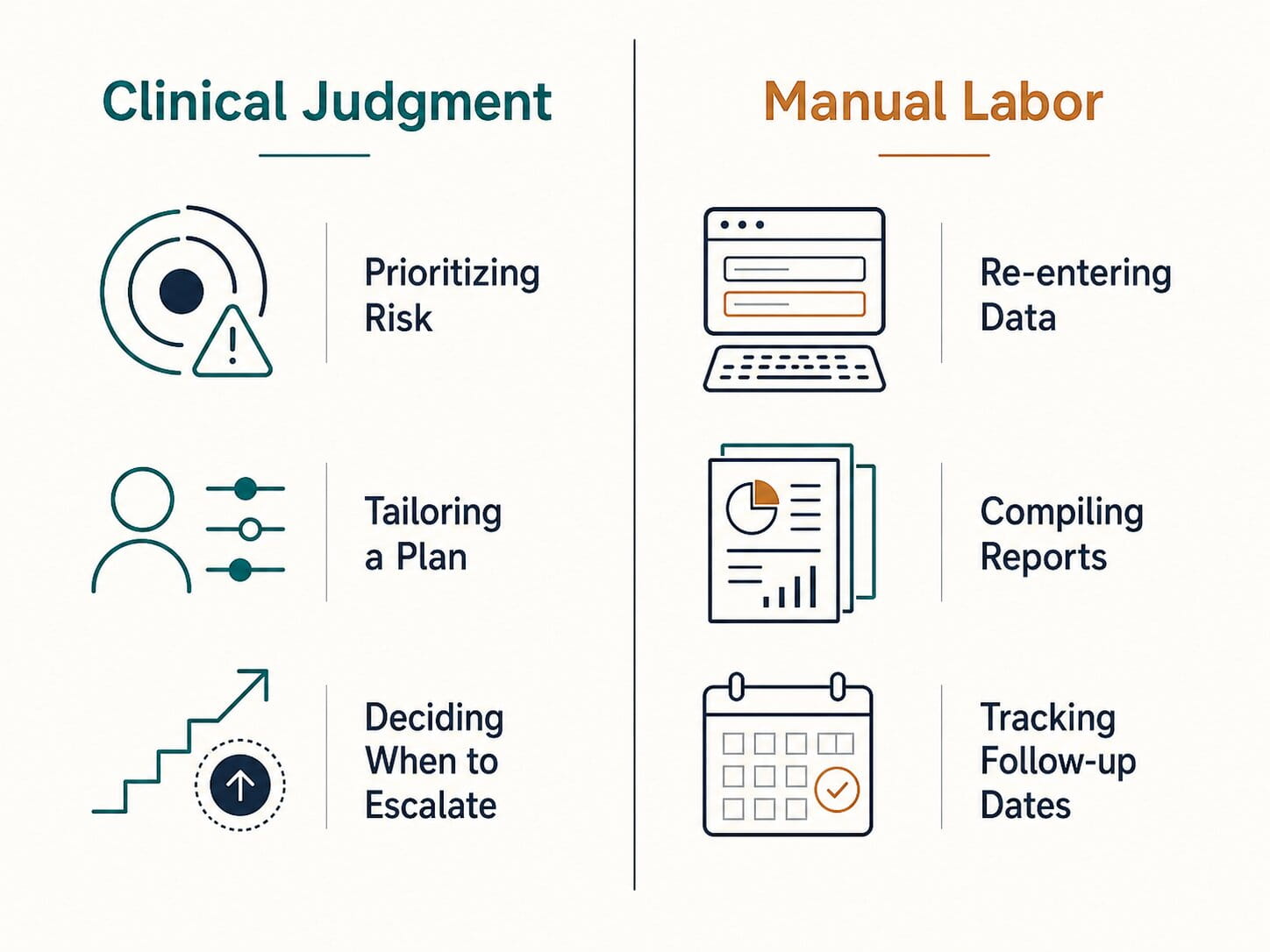
Personalization as clinical judgment includes the decisions that genuinely require an individual clinician synthesizing data against context: prioritizing which findings warrant immediate intervention, tailoring an intervention for a member’s comorbidities or preferences, and deciding when to escalate to specialist referral or additional testing. These decisions cannot be reduced to a rule set, and no clinic should attempt to remove them from clinician control.
Personalization as manual labor includes the work that consumes the same clinician hours but requires none of that judgment: re-entering lab values across systems because they don’t transfer automatically, manually compiling a member’s biomarker trend from three different portals, rebuilding a protocol document from a blank page for every new member, and tracking follow-up dates in a spreadsheet because no system surfaces them automatically.
The reason this distinction matters operationally is straightforward: clinics that conflate the two assume that any attempt to standardize or systematize process threatens clinical quality. In practice, most of what consumes clinician time in a growing longevity practice is the second category, not the first. Confusing manual labor for clinical judgment is what causes clinics to resist the operational changes that would actually protect their ability to scale personalized care — and what causes some clinics to over-correct in the opposite direction, stripping out judgment along with the labor.
Standardization as Governance vs. Standardization as Commoditization
Premium clinics are right to be wary of standardization that flattens their clinical differentiation. But the wariness is often aimed at the wrong target.
Standardization as governance means defining the structure around decisions, not the decisions themselves: consistent pathway stages from intake through outcome review, structured data capture formats so the same biomarker is recorded the same way regardless of which clinician enters it, default retesting cadences for common trajectories, clearly defined role responsibilities across the care team, and — critically — clinician override built into every step. Governance creates consistency in process while leaving the clinical decision itself in the hands of the practitioner.
Integrated care pathway literature supports this distinction: data-driven, structured pathways have been proposed specifically as a mechanism to standardize patient-centered care delivery without removing individualized decision-making. Research from critical care has gone further, finding that standardized, reproducible approaches often produce better outcomes than highly individualized ones for the majority of patients, precisely because reproducibility reduces unintended variation. This evidence comes from acute care settings rather than longevity medicine directly, but the underlying logic — that reproducibility and clinical judgment are not opposites — offers a useful analogue for clinical protocol standardization in longevity and concierge medicine operations.
Standardization as commoditization means removing discretion: identical protocols regardless of individual risk profile, rigid rules that override clinical escalation judgment, and care plans generated without a clinician decision point. This is what premium clinics are correct to reject, and what most fears about “scaling personalized care” are actually about.
The operational task for a growing clinic is not choosing between personalization and standardization. It is building governance — structure around process — while keeping commoditization, which removes judgment, off the table entirely.
What Scalable Personalized Care Requires
Based on the evidence reviewed, several structural requirements separate clinics that scale personalization from those that hit a ceiling.
- Reproducible pathways. A defined sequence of stages from intake through outcome review that every clinician follows, with room for clinical override at each decision point — not a rigid script.
- Role-based task allocation. Clear separation between work that requires a physician, work suited to a nurse or health coach, and work that is purely administrative, so clinical time is not consumed by non-clinical tasks.
- Structured data capture. A consistent format for recording lab, genomic, wearable, and lifestyle data so that information is comparable across members and clinicians, rather than locked in free-text notes or inconsistent spreadsheets.
- Clear follow-up cadence. Default schedules for check-ins, messaging, and retesting based on common member trajectories, adjustable by clinician judgment rather than left undefined by default.
- Longitudinal visibility. The ability to track an individual member’s biomarker trajectory and a program’s aggregate outcomes over time, not just at a single point of care.
- Clinician-controlled protocol decisions. Whatever structure surrounds the workflow, the protocol decision itself — and any deviation from default pathways — must remain with the clinician.
- Consistent documentation of clinical reasoning. Recording not just what was decided but why, so that reasoning is auditable and transferable across a growing team.
- Outcome tracking across members and cohorts. The capacity to demonstrate, at both the individual and program level, whether the care delivered is producing measurable change.
None of these requirements eliminate clinical judgment. Each one is designed to remove the manual labor surrounding that judgment, so clinician time is spent on decisions that actually require a clinician — and so clinic scalability becomes a function of process design rather than founder availability.
Frequently Asked Questions
Why does personalized longevity care struggle to scale?
It struggles to scale when personalization is delivered through one clinician’s manual labor and tacit judgment rather than through a documented, repeatable workflow that a growing team can execute consistently.
Is standardization the same as commoditizing personalized care?
No. Governed standardization structures the process around a clinical decision — pathway stages, data formats, retesting cadence — while leaving the decision itself with the clinician. Commoditization removes clinical discretion entirely, which is a different and avoidable outcome.
What is the biggest hidden bottleneck in longevity clinic operations?
Follow-up, adherence monitoring, and retesting are frequently the largest source of unscheduled clinician workload, more so than the initial consultation or diagnostics ordering stage.
Does adding biomarker panels and wearables make clinics harder to scale?
They can, in the absence of structured data capture. Multi-source data — labs, genomics, wearables, lifestyle inputs — increases interpretive workload faster than most clinics’ systems can organize it, which is a data complexity problem distinct from clinical complexity.
Can a longevity clinic scale without losing clinical judgment?
Yes. Evidence on integrated care pathways indicates that reproducible, governed workflows can coexist with — and in some respects strengthen — individualized clinical decision-making, provided clinician override remains built into the process.
Diagnostic Questions for Clinical Leaders
Clinics evaluating where their own model sits on this spectrum should be able to answer the following with specificity, not generality:
- If a new clinician joined your team tomorrow, could they follow your existing intake-to-outcome process without your direct supervision?
- How much of your senior clinicians’ time each week is spent on biomarker interpretation and protocol design, versus re-entering or reconciling data across systems?
- Do your retesting intervals follow a defined default, or are they decided case by case with no documented rationale?
- If asked to show a member’s or a program’s outcome trajectory over the past twelve months, how long would it take your team to produce that, and from how many systems would the data need to be pulled?
- Where in your current workflow is clinical judgment actually being exercised — and where is it simply unmanaged manual work that happens to require a clinician’s time?
These questions are diagnostic, not rhetorical. The answers indicate whether a clinic’s scaling constraint is clinical, operational, or both — and that distinction determines what kind of structural change is actually needed.
The clinics that scale personalized longevity care are not the ones that personalize less. They are the ones that have separated judgment from labor clearly enough to govern the labor without governing the judgment. That distinction is operational, not philosophical — and it is the one most growing clinics have not yet made explicit.
HolistiCare provides clinical decision-support infrastructure; it is not a licensed medical provider or electronic health record. All diagnostics, care protocols, and clinical decisions remain exclusively the responsibility of qualified healthcare professionals. Insights generated by HolistiCare’s AI engine are for clinical and informational use only and do not constitute medical advice, diagnosis, or treatment.