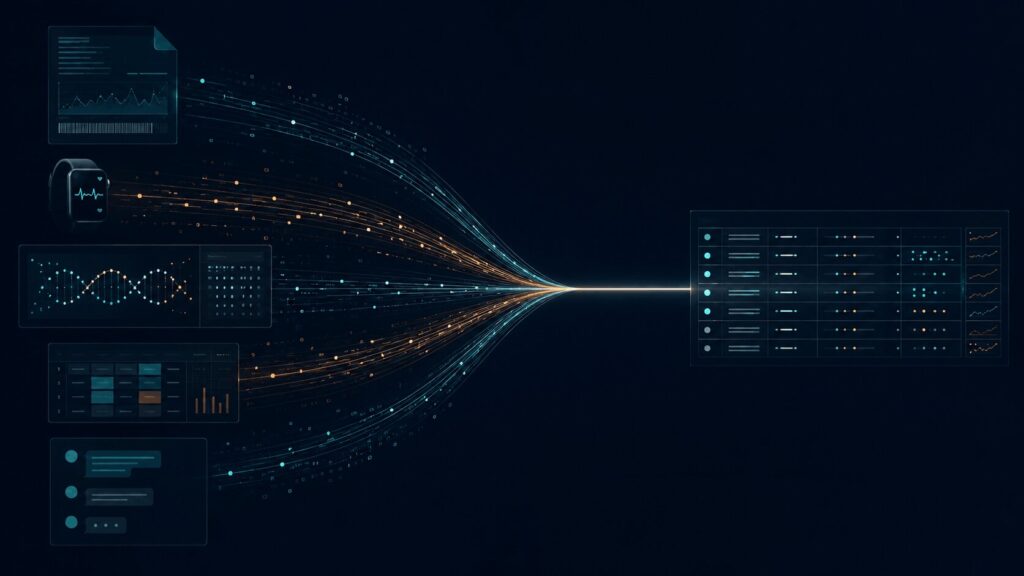
A member arrives for their quarterly review. They completed an intake assessment six weeks ago. They have run a comprehensive cardiometabolic panel, a hormone panel through a specialty lab, and a microbiome assessment. Their wearable data spans ninety days. Their prior genomic report sits in a document folder. Their supplement protocol lives in a dispensary platform. Their follow-up messages are spread across a portal and a secure messaging thread.
The data exists. There is no shortage of it.
The problem is that none of it lives in the same place. Longevity clinic data fragmentation is the condition in which a member’s clinical record is spread across multiple disconnected systems, formats, and portals: present in full, but not structured into one operational record. The clinician reviewing this member today will open several systems, log into multiple portals, read through PDF attachments, cross-reference a spreadsheet, and mentally assemble a longitudinal picture that no single tool has constructed for them. For many longevity, concierge, and functional medicine clinics operating across multiple point tools, this is a familiar workflow.
In brief
- Longevity clinics generate more types of data (labs, genomics, wearables, intake, supplements, messaging) than traditional clinical systems were designed to manage.
- Fragmentation occurs because each data source lives in a different system, format, and portal. No single tool assembles the full member record.
- Adding more point tools typically compounds fragmentation rather than resolving it.
- Fragmented data creates operational burden: higher clinician prep time, inconsistent protocols, weak adherence visibility, and limited capacity to prove clinical outcomes.
- The solution is not a better dashboard. It is a Clinical OS layer: governed operating infrastructure that connects data to workflow, protocol design, and longitudinal outcome reporting.
Longevity Clinics Create More Data Than Traditional Systems Were Built to Manage
Standard ambulatory EHRs were designed for episodic, problem-list, billing-centric care. A visit generates a note, a diagnosis code, a prescription, and a standard lab order. The model is transactional. It was built around the clinical encounter, not the longitudinal member.
Longevity medicine operates on different architecture. A single member program may involve advanced cardiometabolic panels, hormone and metabolic testing, genetic and pharmacogenomic data, microbiome assessments, continuous wearable streams, structured intake questionnaires, personalized supplement protocols, lifestyle coaching, and multi-month follow-up monitoring. Each of these data channels arrives from a different source, in a different format, on a different schedule.
The mismatch between that clinical reality and the infrastructure most clinics have inherited is not a configuration problem. It is structural. Generic EHRs were not built to represent longitudinal biomarker trends, functional medicine timelines, or multi-source data models as first-class clinical objects. Clinics using them for longevity programs are pushing a system beyond the purpose it was designed for.
Where the Fragmentation Starts
EHR and Clinical Notes
The EHR remains the chart of record. In a longevity clinic, it typically captures visits, prescriptions, and basic lab results. Specialty panels, functional assessments, and wearable data rarely map cleanly into its data model. Context is locked in free-text notes. Biomarker trending across time requires manual extraction. The EHR records what happened at each visit. It rarely shows what changed across the program.
Lab Portals and PDF Reports
Conventional lab integration covers large reference labs via structured results messages. Specialty longevity labs (hormones, organic acids, advanced cardiometabolic markers, and others) often have limited integration options, delivering results through separate portals or as PDF attachments. Each portal requires its own login. Units and reference ranges vary across vendors. When results cannot be pulled into a structured format, they are reviewed manually and summarized in notes: a process that adds time and introduces transcription risk at every step.
Genomics and Pharmacogenomics Data
Genomic and pharmacogenomic results are typically delivered as narrative documents or PDFs. Current EHR data models only partially support structured genomic data, with inconsistent nomenclature across vendors and limited clinical decision support integration. For longevity clinics incorporating genomics-informed protocols, the practical consequence is that genomic insights remain point-in-time documents rather than active clinical inputs linked to medications, interventions, and longitudinal outcomes.
Microbiome and Functional Diagnostic Data
Microbiome vendors use proprietary panels and scoring indices. Standards for structured data exchange are still evolving, and most output arrives as graphical PDFs interpreted through vendor-specific frameworks. Trending microbiome metrics over time, or correlating them with dietary interventions and clinical outcomes, requires manual interpretation and cross-document comparison. The evidence base and standardization for these data types continue to develop. Clinics incorporating microbiome testing face the same fragmentation challenge as with any proprietary, PDF-dependent data source.
Wearables and Continuous Vitals
Wearables generate continuous physiologic data: sleep, HRV, resting heart rate, glucose trends, activity patterns. That data aggregates in consumer apps and device dashboards, not in the clinical record. Clinicians typically see high-level summaries at the point of review rather than structured trend views integrated into the member’s longitudinal record. The signal is present. Its connection to protocol decisions and clinical follow-up is largely manual.
Intake Forms and Questionnaires
Longevity and functional medicine programs depend on comprehensive intake: history, lifestyle factors, symptom patterns, antecedents. These are often collected through standalone tools, member portals, or static forms. They do not map into the EHR as structured, queryable data. Clinicians re-gather context at each visit. The intake data that could inform protocol design and cohort analysis sits disconnected from the clinical workflow.
Supplement and Pharmacy Workflows
Supplement and nutraceutical protocols are typically managed through separate dispensary platforms. What a member is prescribed and what they are actually taking are often recorded in different places. Adherence patterns and refill behavior are not linked to biomarker changes in the clinical record. Protocol delivery is fragmented from protocol evidence.
Messaging, Coaching, and Follow-Up Systems
Longevity programs deliver value between visits: through secure messaging, coaching check-ins, remote monitoring, and behavior change support. These interactions happen across portals, telehealth platforms, and in some cases consumer messaging channels. The follow-up record is incomplete. The audit trail for what support was provided, and how a member responded, rarely appears in full in the clinical system.
Spreadsheets and Manual Trackers
When the clinical system cannot answer basic questions (which members improved their metabolic markers in ninety days, which protocols are driving the best adherence) clinics build their own trackers. Spreadsheets become shadow systems. They diverge from the clinical record over time, introduce version control problems, and create governance exposure. They are a rational response to absent infrastructure, and a reliable sign that the infrastructure gap is structural.
Why More Tools Often Create More Fragmentation
The instinct when a data problem appears is to add a tool. A lab aggregator for specialty testing. A wearable hub for device data. A supplement platform for fulfillment. A CRM for the membership journey. A dashboard for analytics.
Each tool solves a slice of the problem. Each tool also adds another data location, another format, another set of credentials, and another layer of manual reconciliation. The stack grows. The coherence does not.
Many current-generation longevity clinics operate across precisely this kind of distributed tool environment and find that the fragmentation is compounded, not resolved, by the additions. Each integration requires maintenance. Each new data source creates another gap in the longitudinal record. The aggregate result is more systems to monitor and fewer clear answers about what is happening with a member’s health over time.
The Operational Cost of Fragmented Data
This is where fragmentation stops being an IT inconvenience and becomes a clinical and commercial constraint.
Clinician time and preparation. Assembling a complete picture of a member before a review requires visiting multiple systems, reading through PDFs, and reconstructing a longitudinal narrative that no single tool has produced. Research on EHR usability confirms that fragmented information across systems significantly increases the time clinicians spend before and during clinical encounters. In high-volume biomarker contexts, that preparation burden can extend considerably: time that is not available for new members or clinical development.
Cognitive load and interpretation quality. When lab results, wearable data, and functional assessments cannot be viewed in a normalized, longitudinal format, each data source must be interpreted in isolation. The clinician holds multiple partial pictures simultaneously and synthesizes them without structural support. More data does not automatically produce better clinical insight. Without a coherent longitudinal model, it can increase cognitive burden rather than reduce it, and introduce interpretive inconsistency across the team.
Protocol consistency. Without structured templates that link biomarker profiles to protocol components, clinicians design programs idiosyncratically: documented in free-text notes, adjunct tool exports, or separate dispensary records. Medical directors cannot reliably enforce standard-of-care pathways, compare protocol performance across the team, or onboard new clinicians into a consistent methodology. Clinical variability is not always visible until it affects outcomes.
Care-team coordination and follow-up. Fragmented messaging, portal data, and task records prevent the care team from maintaining a unified view of a member’s status. Follow-up commitments made in one channel may not appear in the clinical record. Coaching interactions and behavior change data are disconnected from clinical outcomes. Members may receive inconsistent communication from different team members working without a shared view.
Adherence visibility. Whether a member is following their prescribed protocol (supplements, lifestyle interventions, monitoring requirements) is a primary determinant of outcome in longevity medicine. Without a system that connects prescription, delivery, and behavior monitoring in a structured way, adherence is assessed retrospectively through member self-report rather than tracked continuously.
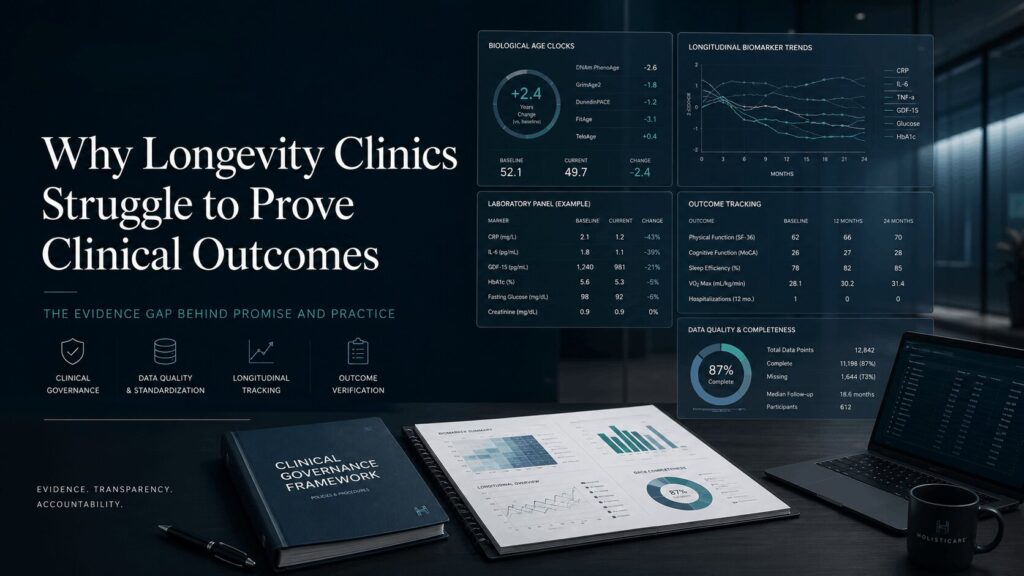
Outcome reporting and auditability. When key data elements are stored as PDFs, notes, or spreadsheets, clinics cannot produce clean, auditable longitudinal outcome reports. The ability to prove clinical outcomes to members, employer partners, or a clinical governance board depends on data that is present but inaccessible in structured form. Longevity sector consensus efforts have specifically highlighted that full data integration and shared standards remain limited in current practice, constraining the field’s ability to produce robust longitudinal evidence.
Member perceived value. For members paying premium program fees, a fragmented experience (multiple logins, inconsistent report formats, the absence of a coherent narrative of progress) erodes perceived value regardless of the clinical work done behind the scenes. A member who cannot see their longitudinal story clearly may underestimate the program’s impact, regardless of what the underlying data shows.
Why This Becomes a Scale Ceiling
A clinician-founder operating with a small member panel can often manage this fragmentation manually. They know the systems. They hold the context. They carry the synthesis capability in their heads and their habits.
This model does not scale.
Add more members, and preparation time becomes unsustainable. Add more clinicians, and protocol inconsistency becomes structural. Add a second location, and governance across the program becomes difficult to maintain. Add an employer health contract or a partnership program, and the demand for auditable longitudinal outcome data requires a level of data infrastructure that manual spreadsheets cannot provide.
The fragmentation that is manageable in a small founder-led program becomes an operating ceiling as the clinic adds more members, clinicians, programs, and locations. What was a workflow inconvenience becomes a structural limit on the program’s capacity, quality, and commercial development.
What Mature Clinics Do Differently
Clinics that have moved beyond this ceiling tend to have made two distinct investments. The first is in data architecture: an intentional approach to how member data is collected, normalized, and stored so that it can be queried, trended, and connected to outcomes. The second is in clinical model standardization: defined biomarker panels, structured protocol templates, shared definitions of what progress looks like, and governed workflows that new clinicians can enter without a long apprenticeship in the founder’s methodology.
These two investments compound. When incoming data maps into consistent structures, and when clinical decisions are built on shared protocol logic, the program becomes something that can be operated rather than improvised. The longitudinal member record (a single, governed, continuously updated clinical record for each member spanning all data sources and time points) becomes a real asset rather than a scattered archive of past encounters.
This is not primarily a technology question. It is an operating model question. But it requires operating infrastructure to support it.
Why This Requires an Operating Layer, Not Another Dashboard
A dashboard can visualize fragmented data. It can pull in results from multiple sources and display them in a single interface. That is useful. It is not sufficient.
The gap in longevity clinic operations is not a visualization gap. It is a workflow gap. Data needs to be connected not just to a screen, but to clinical protocol design, to structured review, to follow-up task management, to governance controls, and to longitudinal outcome reporting. A dashboard that sits on top of disconnected source systems inherits the fragmentation underneath it. The data may be visible. It is not operational.
What longevity clinics operating at scale need is a longevity clinic operating system: a Clinical OS, meaning governed operating infrastructure that creates a normalized, longitudinal member record, connects that record to protocol logic and clinical decision support, routes every decision through a clinician-in-the-loop review process, maintains a full audit trail of clinical actions, and produces structured outcome visibility at both member and cohort level.
The distinction is precise: a dashboard shows what the data says. A Clinical OS layer connects the data to what happens next, across interpretation, protocol design, care-team coordination, and outcome reporting.
How HolistiCare Fits Into This Operating Model
HolistiCare is the Clinical OS built for premium longevity, concierge, and functional medicine clinics. It is not an EMR. It is not a wellness application. It is not an autonomous AI system. It is the operating infrastructure layer designed to consolidate multi-source member data into a governed longitudinal record and connect that record to structured clinical workflow, protocol delivery, and outcome visibility.
HolistiCare is designed to consolidate data across labs, genomics, wearables, intake assessments, and clinical notes into a governed longitudinal member record. A longevity-trained AI engine applies structured interpretation across that record, mapping biomarker data to the clinic’s own protocol templates and generating editable, evidence-based care plan drafts for clinician review. No protocol reaches a member without explicit clinician approval. The AI augments the clinician’s judgment. It does not operate independently of it.
The protocol engine encodes the clinic’s own methodology (its biomarker panels, its intervention logic, its definitions of clinical progress) into a governed, repeatable system. Medical directors can review protocol consistency across the care team. Governance is built into the architecture: every clinical decision creates an audit trail, and role-based access controls manage care-team workflows. Longitudinal outcome data is structured for member-level reporting and cohort-level program analysis, giving clinic founders and medical directors the visibility their programs require.
Frequently Asked Questions
What is longevity clinic data fragmentation?
Longevity clinic data fragmentation is the condition in which a member’s clinical record is spread across multiple disconnected systems, including EHRs, specialty lab portals, PDF reports, wearable dashboards, intake forms, supplement platforms, and messaging tools, rather than consolidated into a single governed longitudinal record. The data exists in full, but is not structured into one operational view. This makes biomarker interpretation, protocol consistency, care-team coordination, adherence monitoring, and outcome reporting significantly harder to execute at scale.
Why do EHRs struggle with longevity clinic data?
Standard ambulatory EHRs were built for episodic, billing-centric, problem-list care. They were not designed to represent longitudinal biomarker trends, functional medicine timelines, multi-vendor specialty lab data, or wearable streams as structured clinical objects. Longevity and functional medicine programs rely on exactly these data types, tracked across months or years and linked to personalized protocols. The mismatch is architectural, not a configuration gap. Clinicians working within standard EHRs for longevity care typically resort to free-text notes, PDF attachments, and external spreadsheets to manage what the EHR cannot model natively.
Why do lab PDFs create operational problems for longevity clinics?
Many specialty labs deliver results as PDF documents rather than structured data. PDFs cannot be trended automatically, queried across a cohort, or linked to protocol templates without manual intervention. Each PDF must be read individually, summarized into notes, and cross-referenced with other data sources by the reviewing clinician. In a longevity clinic running multiple specialty panels per member across a multi-month program, this creates significant preparation burden and limits the clinic’s ability to generate auditable longitudinal outcome reports.
How does fragmented data affect outcome reporting in longevity clinics?
When clinical data is distributed across PDFs, notes, separate portals, and spreadsheets, clinics cannot assemble clean, structured, auditable longitudinal outcome reports. The biomarker changes, protocol adherence records, and follow-up interactions that would demonstrate program value to a member, an employer partner, or a clinical governance board exist but are inaccessible in structured form. This weakens the clinic’s ability to prove clinical outcomes, differentiate its programs with evidence, or negotiate credibly with institutional partners.
What is the difference between a dashboard and a Clinical OS layer?
A dashboard aggregates and visualizes data from multiple sources in a single interface. It solves a visibility problem. A Clinical OS layer goes further: it connects data to clinical workflow, protocol design, structured clinician review, follow-up task management, governance controls, and longitudinal outcome reporting. A dashboard built on top of fragmented source systems inherits the fragmentation underneath it. A Clinical OS layer creates a governed, normalized longitudinal member record that becomes the operational foundation for the clinic’s programs, not just a display layer on top of existing data silos.
Map your clinic's data fragmentation points
Speak with HolistiCare about where member data currently sits across labs, EHRs, wearables, intake forms, spreadsheets, and follow-up workflows, and what a governed Clinical OS layer would consolidate first.
HolistiCare provides clinical decision-support infrastructure; it is not a licensed medical provider or electronic health record. All diagnostics, care protocols, and clinical decisions remain exclusively the responsibility of qualified healthcare professionals. Insights generated by HolistiCare’s AI engine are for clinical and informational use only and do not constitute medical advice, diagnosis, or treatment.
References
-
Ratwani RM, Savage E, Will A, et al. Identifying electronic health record usability and safety challenges in pediatric settings. Health Affairs. 2018;37(11):1752–1759.
-
Gottesman O, Kuivaniemi H, Tromp G, et al. The Electronic Medical Records and Genomics (eMERGE) Network: past, present, and future. Genetics in Medicine. 2013;15(10):761–771.
-
Manolio TA, Chisholm RL, Ozenberger B, et al. Implementing genomic medicine in the clinic: the future is here. Genetics in Medicine. 2013;15(4):258–267.
-
Ferrucci L, Gonzalez-Freire M, Fabbri E, et al. Measuring biological aging in humans: a quest. Aging Cell. 2020;19(2):e13080.
-
Collaborators for Longevity Biomarker Translation. Challenges and recommendations for the translation of biomarkers of aging. Nature Aging. 2024.
-
Longevity Biomarker Consortium. Recommendations for biomarker data collection in clinical trials by longevity biomarker consortia. npj Aging. 2025.
-
UCL Population Health Sciences. Study proposes framework to standardize biomarkers of aging and accelerate clinical translation. UCL News. 2024.
-
Longevity.Technology. Longevity clinics urged to adopt shared best practices. 2025.
-
Longevity.Technology. In search of best practices: longevity clinic white paper. 2024.
-
A framework for an effective healthy longevity clinic. Frontiers in Aging. 2024.
-
Toward responsible longevity medicine: Swiss framework for healthy longevity medicine clinics. Aging Medicine. 2025.
-
Fullscript. Integrating Fullscript with your EHR software. Fullscript Support Center. 2024.
-
Health Catalyst. Healthcare data, analytics, and unified ecosystems. Health Catalyst. 2025.
-
Aristotle Metadata. The hidden risk in healthcare data: shadow systems are your blind spot. 2025.
-
Department of Health Abu Dhabi. Healthy Longevity Medicine Clinic Standard. DoH UAE. 2023.