Abstract
The core commercial failure of preventive and functional medicine is not clinical. It is communicative. We excel at measuring oxidative stress, mapping the microbiome, and interpreting multi-panel biomarker arrays. What we have historically failed to do is translate these findings into the economic language that corporate decision-makers require to authorize expenditure.
This brief presents a systematic framework for communicating the ROI of prevention to CFOs, CHROs, and C-Suite executives. It draws on behavioral economics, health outcomes research, and enterprise risk management — the lexicon of those who control the budget. This is not a sales guide. It is an architectural blueprint for building a persuasive clinical argument that withstands institutional scrutiny.
I. The Fundamental Problem: You Are Speaking Clinician to a Bureaucrat
Let us be direct. When a physician walks into a CFO’s office and says, ‘We should screen your executive team for elevated Lp(a) and advanced glycemic markers,’ the CFO hears: cost. An abstract, unquantifiable cost in exchange for an equally abstract, hypothetical future benefit. The CFO is not wrong to be skeptical. That skepticism is, in fact, his job.
The error belongs to us — the clinicians — for speaking the wrong language. We were trained to think in pathophysiology; executives think in risk-adjusted returns. These are not incompatible worldviews. They are simply different dialects of the same underlying logic: minimize downside, maximize upside over a defined time horizon.
The error belongs to us. We were trained to think in pathophysiology. Executives think in risk-adjusted returns. These are not incompatible — they are different dialects of the same logic.
The first architectural shift required is this: stop framing prevention as a healthcare purchase. Reframe it as what it actually is — a risk management instrument. A structural intervention against known, quantifiable threats to organizational continuity and productivity.
1.1 The Cognitive Bias You Are Fighting
Understanding why executives default to skepticism requires a brief detour into behavioral economics. Nobel laureate Daniel Kahneman’s research on loss aversion is instructive here. Humans are approximately twice as sensitive to losses as to equivalent gains [1]. This means that the promise of a future benefit — even a large one — is psychologically less motivating than the avoidance of an equivalent certain cost.
Prevention, however, deals almost exclusively in future benefits that feel probabilistic. We are asking an executive to spend real money today against a disease state that may never manifest. The cognitive friction is enormous.
The corrective strategy: convert the probabilistic future benefit into a near-certain present cost avoidance. We do not sell the hope of health. We quantify the cost of its current, demonstrable erosion.
1.2 What Executives Actually Measure
Before constructing your economic argument, you must understand the metrics that determine budget allocation decisions in mid-to-large enterprises:
- Total Cost of Risk (TCOR): The aggregate of all costs associated with managing risk — insurance premiums, retained losses, administrative costs. A metric that CFOs and Risk Officers monitor closely.
- Human Capital ROI (HC-ROI): Revenue per employee, output per compensation dollar. This is the lens through which CHROs evaluate workforce investment programs.
- Presenteeism Index: The productivity loss attributable to employees working while sub-optimally healthy. Studies suggest presenteeism costs U.S. employers $1,685 per employee annually in excess of absenteeism [2].
- Executive Replacement Cost: The fully loaded cost of replacing a senior leader — estimated at 200-400% of annual compensation when search fees, onboarding, and productivity loss are calculated [3].
- Group Benefits Claims Trend: The year-over-year trajectory of healthcare claims, which directly impacts insurance renewal pricing. Adverse trend is a tangible, auditable line item.
These are not soft metrics. They are numbers that appear in board presentations and audit documents. Your clinical intervention must be able to demonstrate measurable impact on at least two of these five categories.
II. The Architecture of a Compelling Prevention ROI Case
We have developed what we call the Three-Layer ROI Stack at HolistiCare. It is a structured framework for building an economic case that survives CFO-level interrogation. Each layer adds evidentiary weight and addresses a different objection.
The Three-Layer ROI Stack: Hard Economics, Actuarial Risk Reduction, and Organizational Optionality. Build all three. Present all three.
Layer 1: Hard Economic Quantification
Begin with what is measurable and irrefutable. The objective here is to anchor the conversation in numbers the executive already trusts.
The framework for this layer is straightforward:
- Identify the current cost burden. Pull the prior 36 months of group benefits claims data. Segment by diagnostic category: cardiovascular, metabolic, musculoskeletal, oncological. Calculate the average annual spend per employee in each category.
- Project the trend trajectory. Healthcare claims trend nationally at 7-9% annually [4]. Apply this to the current baseline. Show the executive what inaction costs — not in clinical terms, but in actuarially projected dollar terms over three and five years.
Introduce the intervention cost as a deflator. Present the cost of a comprehensive executive health program not as a new expense, but as a reduction in the projected trend line. If a 5-year projected trend adds $2.8M to group healthcare costs, and a structured prevention protocol costs $400K over the same period, the ROI framing writes itself.
This approach, grounded in actuarial modeling, is the primary language of insurance carriers and risk managers — the very people your executive already trusts with large sums of money.
Layer 2: Actuarial Risk Reduction Through Biomarker Surveillance
The second layer moves from claims data to prospective clinical data. This is where the value of a system like HolistiCare’s Clinical Intelligence Layer becomes structurally apparent — because this layer requires the ability to aggregate, interpret, and trend longitudinal biomarker data at a population level.
The argument is straightforward: the earlier you detect a metabolic, cardiovascular, or oncological trajectory, the less it costs to correct. This is not philosophy — it is health economics.
A practical example to use in executive conversations:
The table above does the heavy lifting for you. Early detection is not a clinical nicety — it is a cost compression strategy. Present it that way.
The HolistiCare platform operationalizes this layer by ingesting lab data via OCR, correlating biomarker trajectories across panels, and surfacing early-signal alerts that legacy EHR systems — designed for documentation, not intelligence — will categorically miss. The delta between detection at Stage A versus Stage C is not a clinical outcome metric. It is a budget line item
Layer 3: Organizational Optionality and Strategic Resilience
The third layer is the most sophisticated and often the most persuasive for senior executives who think in strategic time horizons. It moves beyond cost avoidance into the territory of competitive advantage.
The argument: The health of your senior leadership team is a strategic asset. Its degradation is a material risk. Few organizations manage it as such.
Consider the following vectors of organizational optionality that a structured executive health program protects:
- Key-Person Dependency Risk: If your CFO, CTO, or Founder experiences a major cardiovascular event at 54, what is the organizational and market impact? This is not a morbid hypothetical — it is a risk scenario that boards and investors increasingly require disclosure on.
- Cognitive Performance as a Competitive Moat: Emerging research on neurological biomarkers — including inflammatory cytokines, cortisol-DHEA ratios, and sleep architecture metrics — demonstrates measurable correlation with executive decision-making quality [5]. Poor metabolic health is a cognitive tax on the organization’s most expensive talent.
- Retention Signal: Structured executive health programs function as a high-signal retention mechanism. In a market where replacing a VP-level hire costs 200-400% of annual compensation, an investment in a comprehensive health program costing $15,000–$30,000 annually per executive requires roughly 3-5% retention improvement to break even. Data from Society for Human Resource Management research suggest these programs routinely outperform that threshold [6].
- Insurance and Actuarial Favorability: Organizations demonstrating proactive health risk management increasingly qualify for favorable group insurance underwriting. Some carriers offer experience rating credits for documented wellness program participation — a direct, auditable financial return.
III. The Clinical Friction Problem in Institutional Health Programs
Here we must address an internal failure mode that clinical operators often overlook. Even when the economic case is accepted and a corporate health program is approved, implementation frequently collapses under what we term Clinical Friction — the accumulated inefficiencies, communication failures, and data silos that prevent a program from delivering on its promised ROI.
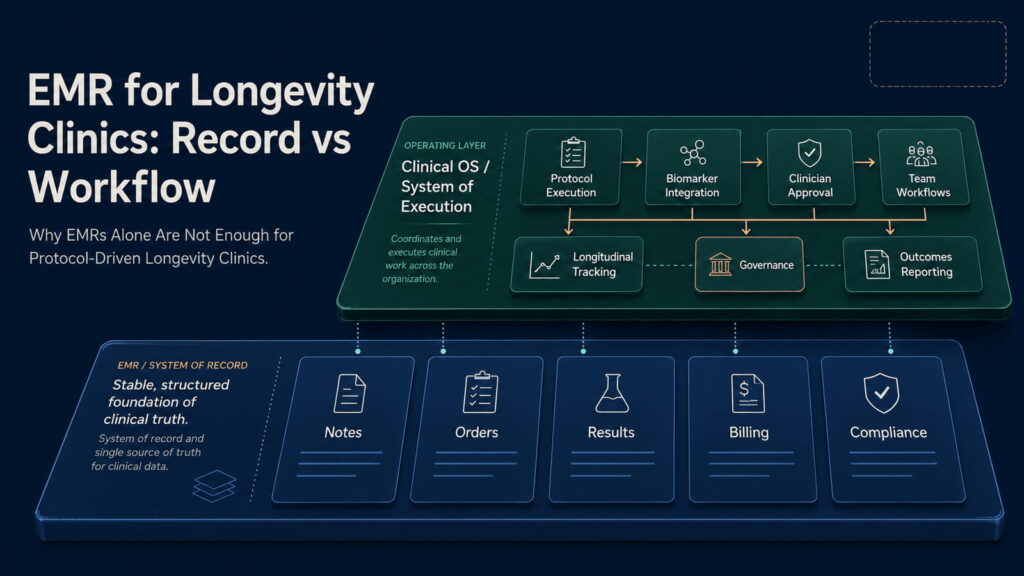
This is precisely where legacy EHR infrastructure becomes an active liability rather than a neutral administrative tool. Cerbo, Practice Better, Charm, and their contemporaries are — architecturally speaking — filing cabinets. Sophisticated, cloud-accessible filing cabinets, but filing cabinets nonetheless. They were designed to document clinical encounters and manage billing. They were not designed to synthesize data, detect biomarker trends, or produce the kind of outcome dashboards that a CFO expects to see at a quarterly review.
Legacy EHRs were designed to document clinical encounters. The CFO does not care about documentation. The CFO cares about the dashboard — the outcome trend, the ROI delta, the early-warning signal. That requires Clinical Intelligence, not a filing cabinet.
We do not abandon legacy infrastructure — we integrate with it. HolistiCare’s Clinical Intelligence Layer sits atop your existing EHR, ingesting its data, augmenting it with OCR-processed external lab results, and transforming raw clinical records into actionable population health insights.
The output is what executives actually need to justify continued investment: a clean, auditable record of clinical intervention, biomarker trajectory, risk profile change, and projected cost avoidance. This is not a physician’s chart note. This is a fiduciary document.
3.1 The Cognitive Load Tax on Your Clinical Team
There is a secondary problem that Clinical Friction imposes — one that affects not the executive buyer, but the clinical operator delivering the program. When physicians spend hours manually correlating lab results across systems, constructing narrative summaries for non-clinical stakeholders, and managing the administrative overhead of a corporate wellness program through a documentation-first EHR, the result is predictable: burnout, error, and eventual program deterioration.
This is the Hero Trap applied to institutional medicine. The program’s quality becomes dependent on the extraordinary effort of individual clinicians rather than the systematic intelligence of the infrastructure. It does not scale. And when the lead physician burns out or transitions, the program collapses with them.
Systematization is not a compromise of the art of medicine. It is the precondition for its sustainable delivery at institutional scale.
IV. The Conversation Framework: Speaking Executive to Executive
The following is a structured conversation framework we provide to HolistiCare partner clinicians when they are presenting to corporate buyers. It is not a script. It is a decision tree designed to navigate the predictable objections.
Phase 1: Establish Common Ground (Minutes 1-5)
Do not open with clinical data. Open with organizational risk. Your entry point should be one of the following:
- “I’d like to discuss how peer organizations in your sector are treating executive health as a risk management function rather than a benefits line item — and what the financial outcomes have looked like.”
- “I’ve been looking at your group healthcare claims trend, and I want to show you a 5-year projection that I think will be relevant to your next renewal conversation.”
- “Two of your direct competitors have implemented structured executive health protocols in the last 18 months. I can walk you through what their CFOs told me about the actuarial outcomes.”
These openers establish clinical credibility through business framing. You are signaling that you understand the room.
Phase 2: Surface the Hidden Costs (Minutes 5-15)
Introduce the Presenteeism Paradox: the most expensive health costs your organization is bearing right now are invisible. They appear on no claims report. They show up in missed deadlines, suboptimal decisions, and leadership fatigue.
Use concrete numbers. The Harvard Business Review has published extensively on the cost of untreated chronic stress and metabolic dysfunction in knowledge workers [7]. A senior executive operating at 75% cognitive capacity due to sleep dysregulation and subclinical insulin resistance is not a clinical problem — it is a $400,000-per-year productivity problem.
Allow this to land. Do not immediately offer the solution. Let the executive process the cost of the status quo.
Phase 3: Present the System, Not the Service (Minutes 15-30)
The most common mistake clinicians make in this phase is pivoting to a menu of services: lab panels, consultations, supplements. This immediately reframes the conversation as a healthcare transaction — the exact framing you have worked to escape.
Instead, present a system. A protocol-driven, data-generating, outcome-measuring infrastructure that will produce quarterly reports your CFO can present to the board. Emphasize the following:
- Baseline Biomarker Architecture: We establish a comprehensive baseline for each participating executive across metabolic, cardiovascular, hormonal, neurological, and inflammatory domains. This becomes the organizational risk register.
- Longitudinal Trend Intelligence: Unlike a single annual physical, our protocol generates continuous trend data. We detect drift before it becomes event. This is the difference between reactive and predictive medicine.
- Outcome Reporting Stack: Quarterly executive summaries, annual actuarial review, and direct integration with your HR and benefits infrastructure. Everything your organization needs to demonstrate ROI to insurers and board members.
Phase 4: Handle the Four Standard Objections
Objection 1: “Our current benefits plan already covers physicals.”
Response: “It does — and we integrate with it. What your benefits plan offers is a diagnostic snapshot: a single data point, once per year, interpreted against population norms. What we build is a longitudinal intelligence system interpreted against each executive’s individual baseline and trajectory. These are architecturally different products. One documents the present. The other predicts and prevents the future.”
Objection 2: “How do we measure ROI on something that doesn’t happen?”
Response: “The same way your insurance carrier does — through actuarial modeling. We document the baseline risk profile, we document the intervention, and we document the trajectory change. We can calculate the cost of each prevented escalation using nationally validated healthcare cost databases. This is not medicine on faith — it is medicine on data. We will give you the same evidence standard your CFO uses for any other risk mitigation investment.”
Objection 3: “This feels like a perk for the C-suite, not a business investment.”
Response: “I understand the perception — and it’s worth addressing directly. We are not proposing a spa day with a blood draw. We are proposing a structured risk management protocol applied to your organization’s highest-cost, highest-impact human capital assets. Would you decline to insure your most valuable physical assets because it looked like a perk? Executive health infrastructure follows the same fiduciary logic.”
Objection 4: “We’ve tried wellness programs before and they didn’t move the needle.”
Response: “I’d want to understand what you tried — because the category of ‘wellness program’ spans from gym memberships to clinically-structured biomarker surveillance. The former has weak evidence. The latter has strong health economics literature. The programs that fail are typically engagement-based: they rely on voluntary participation and self-reported outcomes. What we build is protocol-based — data-mandatory, clinician-interpreted, and outcome-auditable. These are categorically different architectures.”
V. The Data Infrastructure Imperative
Notably, all recorded key events correspond to inbound demo requests, with approximately 2.6% of total users converting into demo requests, indicating that a measurable and growing share of incoming traffic is highly intent-driven and actively evaluating the product.
The preventive medicine physician who attempts to build a corporate health program on top of a documentation-first EHR will discover a fundamental mismatch. Legacy systems produce chart notes. Corporate health programs require population dashboards, trend analytics, risk stratification matrices, and ROI calculations. These outputs do not emerge from documentation. They emerge from intelligence.
The HolistiCare Clinical Intelligence Layer was architected specifically to fill this gap. It sits upstream of the EHR, ingesting and correlating data from:
- OCR Lab Ingestion: Automated extraction and normalization of lab data from any external source — Quest, LabCorp, specialty labs — eliminating the manual transcription that introduces both error and delay into traditional workflows.
- Multi-Panel Biomarker Correlation: The ability to surface relationships between biomarker clusters — for instance, correlating elevated hs-CRP with fasting insulin and SHBG to build a comprehensive cardiometabolic risk picture — that no single-panel review would identify.
- Longitudinal Trend Visualization: Patient-facing and clinician-facing dashboards that show trajectory, not just state. Is the executive’s HbA1c trending up 0.3 points per quarter? That is a predictive signal. Legacy systems show you where you are. HolistiCare shows you where you are going.
- Executive Reporting Suite: Aggregated, de-identified population-level reports designed for the CHRO and CFO, not the treating physician. These are the documents that justify renewal of the program budget.
The clinician who can walk into a quarterly review with a CFO and show a dashboard demonstrating measurable risk profile improvement across an executive cohort — correlated to projected claims trend reduction — has transformed the conversation from healthcare expenditure to enterprise risk management. This is the commercial architecture of prevention done correctly.
VI. Implementation: From Concept to Institutional Contract
The final operational question is how to move from compelling conversation to signed agreement. We observe that the most common failure point for clinicians in this space is not the clinical design of the program — it is the commercial architecture.
6.1 Structure the Engagement as a Service Level Agreement, Not a Treatment Plan
Corporate buyers do not purchase treatment plans. They purchase Service Level Agreements (SLAs) — contractually defined deliverables, timelines, and outcome metrics. Your clinical program must be packaged as the latter. Define with specificity:
- What biomarker domains will be surveilled and at what frequency
- What constitutes a reportable event and what is the response protocol
- What outcome metrics will be reported and at what reporting cadence
- What the program’s defined success criteria are at 12, 24, and 36 months
- What the program’s exit and handoff protocols are
This level of operational specificity communicates institutional competence. It signals that you have built a system, not a practice.
6.2 Price to the ROI, Not to the Cost
The final structural error to avoid is pricing your program as a healthcare cost. A comprehensive executive health program that can credibly demonstrate 3:1 ROI through claims trend reduction and productivity preservation should be priced accordingly — not as a per-visit billing code.
The appropriate pricing model for institutional prevention is a per-member-per-year (PMPY) retainer structure, benchmarked against the actuarially projected cost avoidance it delivers. If your program costs $20,000 per executive annually and can demonstrate $60,000 in projected cost avoidance through early detection and protocol adherence, you are selling a 3x return. Price it like that. Present it like that. Contract it like that.
6.3 Build the Proof Stack Before the Conversation
The executives who will approve this investment require social proof from institutional sources. Build your evidence dossier before you walk into the room. It should contain:
- Peer-reviewed health economics literature quantifying the ROI of preventive medicine at the employer level
- Case studies from comparable organizations (anonymized where required)
- Your own program’s outcome data — even from a small initial cohort — presented in actuarial format
- Third-party validation: insurance carrier acknowledgment, actuary letters, or employer coalition endorsements
We at HolistiCare provide our partner clinicians with a curated institutional evidence library that can be white-labeled for their practice’s presentations. The argument should never depend solely on the clinician’s personal credibility. It should be built on structural evidence that persists independently.
VII. Conclusion: The Architecture of Persuasion
Prevention is not a hard sell because executives are irrational. It is a hard sell because clinicians are speaking the wrong language in the wrong room.
The solution is not to simplify the clinical argument. It is to systematize the commercial argument. Build the Three-Layer ROI Stack. Master the Objection Framework. Deploy Clinical Intelligence infrastructure that produces the fiduciary documents your institutional buyers require.
Most importantly, abandon the model in which the quality of the program depends on the heroic individual effort of a single physician maintaining institutional relationships through personal charisma. That model does not scale, and it does not survive the transition of key personnel.
What scales is architecture. A systematized clinical program, supported by intelligent data infrastructure, producing auditable outcomes that speak the language of enterprise risk management. That is what we build at HolistiCare. That is what preventive medicine requires if it is to occupy the institutional position it deserves.
Prevention is not invisible. We have simply been failing to render it visible in the formats that matter.
References
[1] Kahneman, D., & Tversky, A. (1979). Prospect Theory: An Analysis of Decision under Risk. Econometrica, 47(2), 263–291.
[2] Goetzel, R. Z., Long, S. R., Ozminkowski, R. J., et al. (2004). Health, Absence, Disability, and Presenteeism Cost Estimates of Certain Physical and Mental Health Conditions Affecting U.S. Employers. Journal of Occupational and Environmental Medicine, 46(4), 398–412.
[3] Society for Human Resource Management. (2022). The True Cost of Replacing an Employee. SHRM Research Reports.
[4] Health Care Cost Institute. (2024). Health Care Cost and Utilization Report: 2023 Annual Data. HCCI.
[5] Kivimäki, M., & Steptoe, A. (2018). Effects of stress on the development and progression of cardiovascular disease. Nature Reviews Cardiology, 15(4), 215–229.
[6] Society for Human Resource Management & World at Work. (2023). Employee Benefits Survey: Health and Wellness Program ROI. SHRM Publications.
[7] Schwartz, T., & McCarthy, C. (2007). Manage Your Energy, Not Your Time. Harvard Business Review, 85(10), 63–73.
[8] Milani, R. V., & Lavie, C. J. (2009). Reducing Psychosocial Stress: A Novel Mechanism of Improving Survival from Exercise Training. American Journal of Medicine, 122(10), 931–938.
[9] Baicker, K., Cutler, D., & Song, Z. (2010). Workplace Wellness Programs Can Generate Savings. Health Affairs, 29(2), 304–311.
[10] American Diabetes Association. (2024). Economic Standards of Care in Diabetes. Diabetes Care, 47(Suppl 1).
Legal & Medical Disclaimer: This document is produced for educational and informational purposes by HolistiCare.io and does not constitute medical advice, clinical guidance, or a substitute for individualized clinical judgment. The economic projections, ROI calculations, and cost estimates presented herein are illustrative models based on published health economics literature and should be independently validated for any specific organizational context. HolistiCare.io does not guarantee specific clinical or financial outcomes. All clinical protocols should be implemented under the supervision of a licensed healthcare professional. The examples and case scenarios described are hypothetical constructs for illustrative purposes. Readers should consult qualified legal, financial, and clinical advisors before implementing institutional health programs. HolistiCare.io is a clinical intelligence software company and does not provide direct clinical services.